David J Fei-Zhang, Achilles A Kanaris, Camaren M Cuenca, Sydney A Fleishman, Jill N D'Souza, Anthony M Sheyn, Daniel C Chelius, Jeffrey C Rastatter
{"title":"数字不平等对美国口咽癌差异的影响。","authors":"David J Fei-Zhang, Achilles A Kanaris, Camaren M Cuenca, Sydney A Fleishman, Jill N D'Souza, Anthony M Sheyn, Daniel C Chelius, Jeffrey C Rastatter","doi":"10.1002/oto2.70113","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess associations of digital inequity with oropharyngeal cancer (OPC) prognostic and care outcomes in the United States while adjusting for traditional social determinants/drivers of health (SDoH).</p><p><strong>Study design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>United States.</p><p><strong>Methods: </strong>In total, 70,604 patients from 2008 to 2017 were assessed for regression trends in long-term follow-up period, survival, prognosis, and treatment across increasing overall digital inequity, as measured by the Digital Inequity Index (DII). DII is based on 17 census-tract level variables derived from the American Community Survey and Federal Communications Commission. Variables were categorized as infrastructure-access (ie, digital-related variables) or sociodemographic (ie, education, income, and disability status) and weighted-averaged into a composite score.</p><p><strong>Results: </strong>With increasing DII, decreases in length of follow-up (10.22%, 32.9-29.5 months; <i>P</i> < .001) and survival (8.93%, 19-17.3 months; <i>P</i> < .001) were observed. Affordability of internet access displayed the largest influence, followed by device access and internet-service availability. Compared to OPC patients with low digital inequity, high digital inequity was associated with increased odds of diagnosing more than one malignant tumor (odds ratio [OR] 1.01, 95% CI 1.01-1.03; <i>P</i> = .012) and advanced staging (OR 1.01, 95% CI 1.00-1.02; <i>P</i> = .034), while having decreased odds of receiving indicated chemotherapy (OR 0.98, 95% CI 0.97-0.99; <i>P</i> < .001), radiation therapy (OR 0.98, 95% CI 0.97-0.99; <i>P</i> < .001), or primary surgery (OR 0.98, 95% CI 0.97-0.99; <i>P</i> < .001).</p><p><strong>Conclusion: </strong>Digital inequities contribute to detrimental trends in OPC patient care and prognosis in the United States. These findings can inform strategic discourse targeted against the most pertinent disparities in the modern-day environment.</p>","PeriodicalId":19697,"journal":{"name":"OTO Open","volume":"9 2","pages":"e70113"},"PeriodicalIF":1.8000,"publicationDate":"2025-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11980432/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Digital Inequities on Oropharyngeal Cancer Disparities in the United States.\",\"authors\":\"David J Fei-Zhang, Achilles A Kanaris, Camaren M Cuenca, Sydney A Fleishman, Jill N D'Souza, Anthony M Sheyn, Daniel C Chelius, Jeffrey C Rastatter\",\"doi\":\"10.1002/oto2.70113\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To assess associations of digital inequity with oropharyngeal cancer (OPC) prognostic and care outcomes in the United States while adjusting for traditional social determinants/drivers of health (SDoH).</p><p><strong>Study design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>United States.</p><p><strong>Methods: </strong>In total, 70,604 patients from 2008 to 2017 were assessed for regression trends in long-term follow-up period, survival, prognosis, and treatment across increasing overall digital inequity, as measured by the Digital Inequity Index (DII). DII is based on 17 census-tract level variables derived from the American Community Survey and Federal Communications Commission. Variables were categorized as infrastructure-access (ie, digital-related variables) or sociodemographic (ie, education, income, and disability status) and weighted-averaged into a composite score.</p><p><strong>Results: </strong>With increasing DII, decreases in length of follow-up (10.22%, 32.9-29.5 months; <i>P</i> < .001) and survival (8.93%, 19-17.3 months; <i>P</i> < .001) were observed. Affordability of internet access displayed the largest influence, followed by device access and internet-service availability. Compared to OPC patients with low digital inequity, high digital inequity was associated with increased odds of diagnosing more than one malignant tumor (odds ratio [OR] 1.01, 95% CI 1.01-1.03; <i>P</i> = .012) and advanced staging (OR 1.01, 95% CI 1.00-1.02; <i>P</i> = .034), while having decreased odds of receiving indicated chemotherapy (OR 0.98, 95% CI 0.97-0.99; <i>P</i> < .001), radiation therapy (OR 0.98, 95% CI 0.97-0.99; <i>P</i> < .001), or primary surgery (OR 0.98, 95% CI 0.97-0.99; <i>P</i> < .001).</p><p><strong>Conclusion: </strong>Digital inequities contribute to detrimental trends in OPC patient care and prognosis in the United States. These findings can inform strategic discourse targeted against the most pertinent disparities in the modern-day environment.</p>\",\"PeriodicalId\":19697,\"journal\":{\"name\":\"OTO Open\",\"volume\":\"9 2\",\"pages\":\"e70113\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-04-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11980432/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"OTO Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/oto2.70113\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTO Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/oto2.70113","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:评估数字不平等与美国口咽癌(OPC)预后和护理结果的关系,同时调整传统的社会决定因素/健康驱动因素(SDoH)。研究设计:回顾性队列研究。背景:美国。方法:通过数字不平等指数(DII)衡量,2008年至2017年共有70,604例患者接受了长期随访期、生存、预后和治疗的回归趋势评估。DII是基于美国社区调查和联邦通信委员会得出的17个人口普查区水平变量。变量被分类为基础设施访问(即与数字相关的变量)或社会人口统计(即教育、收入和残疾状况),并加权平均成一个综合分数。结果:随着DII的增加,随访时间缩短(10.22%,32.9 ~ 29.5个月;P P = 0.012)和晚期分期(OR 1.01, 95% CI 1.00-1.02;P = 0.034),而接受指征化疗的几率降低(OR 0.98, 95% CI 0.97-0.99;结论:数字不平等导致了美国OPC患者护理和预后的不利趋势。这些发现可以为针对现代环境中最相关的差异的战略话语提供信息。
The Impact of Digital Inequities on Oropharyngeal Cancer Disparities in the United States.
Objective: To assess associations of digital inequity with oropharyngeal cancer (OPC) prognostic and care outcomes in the United States while adjusting for traditional social determinants/drivers of health (SDoH).
Study design: Retrospective cohort study.
Setting: United States.
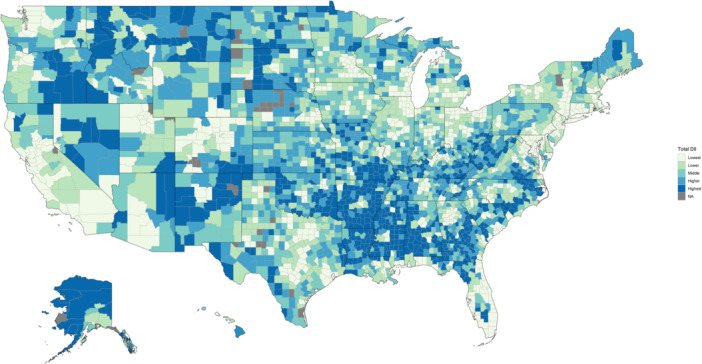
Methods: In total, 70,604 patients from 2008 to 2017 were assessed for regression trends in long-term follow-up period, survival, prognosis, and treatment across increasing overall digital inequity, as measured by the Digital Inequity Index (DII). DII is based on 17 census-tract level variables derived from the American Community Survey and Federal Communications Commission. Variables were categorized as infrastructure-access (ie, digital-related variables) or sociodemographic (ie, education, income, and disability status) and weighted-averaged into a composite score.
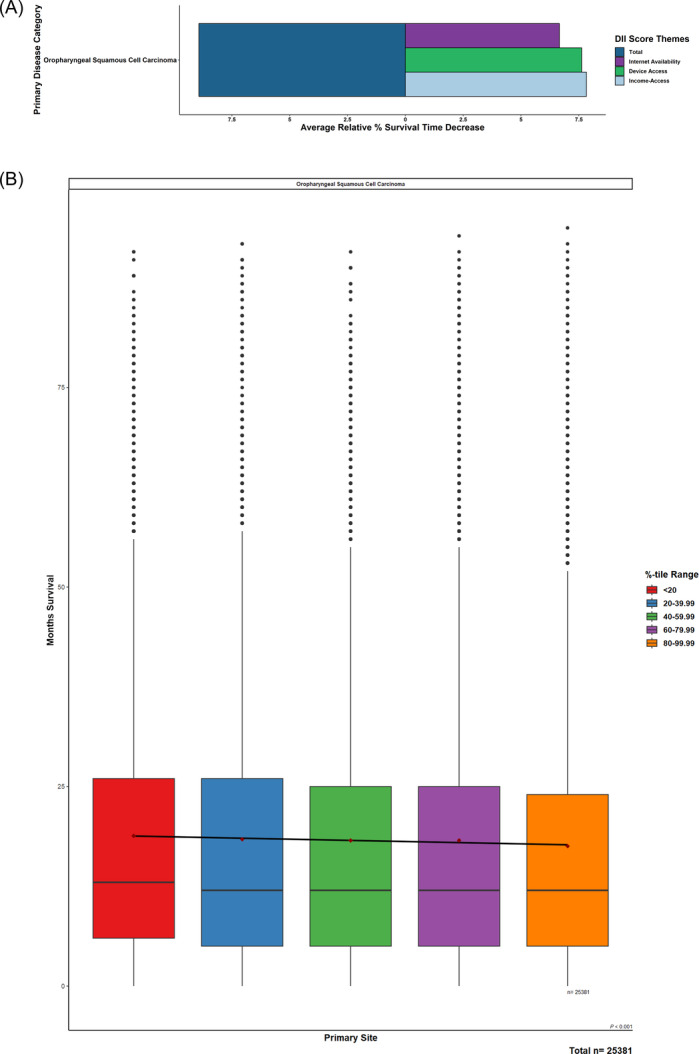
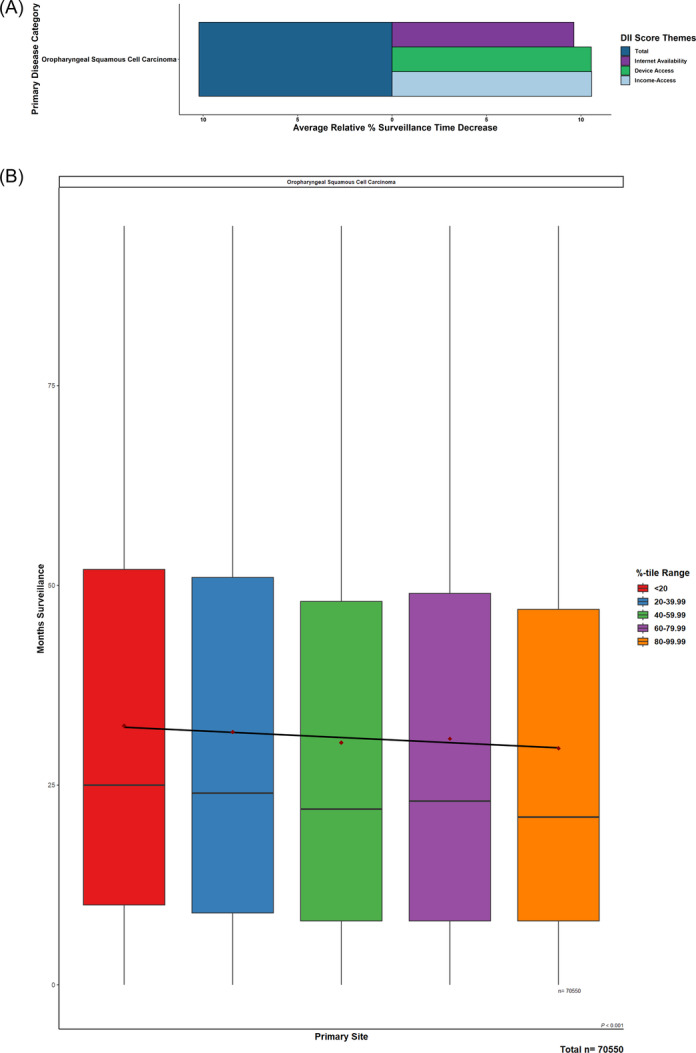
Results: With increasing DII, decreases in length of follow-up (10.22%, 32.9-29.5 months; P < .001) and survival (8.93%, 19-17.3 months; P < .001) were observed. Affordability of internet access displayed the largest influence, followed by device access and internet-service availability. Compared to OPC patients with low digital inequity, high digital inequity was associated with increased odds of diagnosing more than one malignant tumor (odds ratio [OR] 1.01, 95% CI 1.01-1.03; P = .012) and advanced staging (OR 1.01, 95% CI 1.00-1.02; P = .034), while having decreased odds of receiving indicated chemotherapy (OR 0.98, 95% CI 0.97-0.99; P < .001), radiation therapy (OR 0.98, 95% CI 0.97-0.99; P < .001), or primary surgery (OR 0.98, 95% CI 0.97-0.99; P < .001).
Conclusion: Digital inequities contribute to detrimental trends in OPC patient care and prognosis in the United States. These findings can inform strategic discourse targeted against the most pertinent disparities in the modern-day environment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


