Marijn P Mulder, Jan-Willem Potters, Lex M van Loon, Kenny Rumindo, Magnus Hallbäck, Elira Maksuti, Dirk W Donker, Claudius Diez
{"title":"呼气末闭塞试验预测机械通气患者体液反应的临床适用性:一项系统综述和荟萃分析。","authors":"Marijn P Mulder, Jan-Willem Potters, Lex M van Loon, Kenny Rumindo, Magnus Hallbäck, Elira Maksuti, Dirk W Donker, Claudius Diez","doi":"10.1097/EJA.0000000000002181","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The emergence of context-specific clinical evidence from the end-expiratory occlusion test (EEOT) may change the perception of its operative performance to predict fluid responsiveness.</p><p><strong>Objectives: </strong>Assessment of predictive performance of the EEOT in the intensive care unit (ICU) and operating room.</p><p><strong>Design: </strong>Systematic review of observational diagnostic test accuracy studies with meta-analysis.</p><p><strong>Data sources: </strong>MEDLINE, Embase and Scopus were used as data sources for relevant publications until February 2024.</p><p><strong>Eligibility criteria: </strong>Prospective clinical studies in which the EEOT was used to predict fluid responsiveness in mechanically ventilated adults, regardless of the clinical care context. The operative performance characteristics must also have been reported.</p><p><strong>Results: </strong>Twenty-four studies involving 1073 adult patients (588 receiving intensive care and 485 in the operating room) were systematically reviewed, and 22 studies comprising 1049 volume expansions were meta-analysed. The pooled sensitivity [95% confidence interval (CI)] of the EEOT was 0.87 (0.81 to 0.92), and the pooled specificity was 0.90 (0.85 to 0.94); the median [interquartile range] cardiac index ( CI ) threshold for a positive test was a 5.0 [3.3 to 5.3] increase. The clinical context, the method used for haemodynamic monitoring, the ratio of the averaging time of the monitoring method to the occlusion time, the levels of positive end-expiratory pressure and the choice of cardiac output marker were identified as significant sources of heterogeneity. However, the occlusion duration and tidal volume did not significantly affect its performance. A novel insight is that performance was notably lower in the operating room setting. The likelihood ratios were 14 (positive) and 0.12 (negative) for the ICU, both better than 3.1 and 0.21 for the operating room. The overall quality of the evidence was assessed to be very low, mainly due to high heterogeneity and risk of bias; however, no publication bias was detected.</p><p><strong>Conclusion: </strong>The EEOT for predicting fluid responsiveness in critical care performs acceptably well overall and is a confirmative test. In the operating room and/or with specific technical settings, its performance and clinical utility are reduced, driving the need for more context-specific and patient-specific fluid responsiveness assessments.</p>","PeriodicalId":11920,"journal":{"name":"European Journal of Anaesthesiology","volume":" ","pages":"737-746"},"PeriodicalIF":6.8000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237134/pdf/","citationCount":"0","resultStr":"{\"title\":\"Context-specific clinical applicability of the end-expiratory occlusion test to predict fluid responsiveness in mechanically ventilated patients: A systematic review and meta-analysis.\",\"authors\":\"Marijn P Mulder, Jan-Willem Potters, Lex M van Loon, Kenny Rumindo, Magnus Hallbäck, Elira Maksuti, Dirk W Donker, Claudius Diez\",\"doi\":\"10.1097/EJA.0000000000002181\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The emergence of context-specific clinical evidence from the end-expiratory occlusion test (EEOT) may change the perception of its operative performance to predict fluid responsiveness.</p><p><strong>Objectives: </strong>Assessment of predictive performance of the EEOT in the intensive care unit (ICU) and operating room.</p><p><strong>Design: </strong>Systematic review of observational diagnostic test accuracy studies with meta-analysis.</p><p><strong>Data sources: </strong>MEDLINE, Embase and Scopus were used as data sources for relevant publications until February 2024.</p><p><strong>Eligibility criteria: </strong>Prospective clinical studies in which the EEOT was used to predict fluid responsiveness in mechanically ventilated adults, regardless of the clinical care context. The operative performance characteristics must also have been reported.</p><p><strong>Results: </strong>Twenty-four studies involving 1073 adult patients (588 receiving intensive care and 485 in the operating room) were systematically reviewed, and 22 studies comprising 1049 volume expansions were meta-analysed. The pooled sensitivity [95% confidence interval (CI)] of the EEOT was 0.87 (0.81 to 0.92), and the pooled specificity was 0.90 (0.85 to 0.94); the median [interquartile range] cardiac index ( CI ) threshold for a positive test was a 5.0 [3.3 to 5.3] increase. The clinical context, the method used for haemodynamic monitoring, the ratio of the averaging time of the monitoring method to the occlusion time, the levels of positive end-expiratory pressure and the choice of cardiac output marker were identified as significant sources of heterogeneity. However, the occlusion duration and tidal volume did not significantly affect its performance. A novel insight is that performance was notably lower in the operating room setting. The likelihood ratios were 14 (positive) and 0.12 (negative) for the ICU, both better than 3.1 and 0.21 for the operating room. The overall quality of the evidence was assessed to be very low, mainly due to high heterogeneity and risk of bias; however, no publication bias was detected.</p><p><strong>Conclusion: </strong>The EEOT for predicting fluid responsiveness in critical care performs acceptably well overall and is a confirmative test. In the operating room and/or with specific technical settings, its performance and clinical utility are reduced, driving the need for more context-specific and patient-specific fluid responsiveness assessments.</p>\",\"PeriodicalId\":11920,\"journal\":{\"name\":\"European Journal of Anaesthesiology\",\"volume\":\" \",\"pages\":\"737-746\"},\"PeriodicalIF\":6.8000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237134/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Anaesthesiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/EJA.0000000000002181\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Anaesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/EJA.0000000000002181","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Context-specific clinical applicability of the end-expiratory occlusion test to predict fluid responsiveness in mechanically ventilated patients: A systematic review and meta-analysis.
Background: The emergence of context-specific clinical evidence from the end-expiratory occlusion test (EEOT) may change the perception of its operative performance to predict fluid responsiveness.
Objectives: Assessment of predictive performance of the EEOT in the intensive care unit (ICU) and operating room.
Design: Systematic review of observational diagnostic test accuracy studies with meta-analysis.
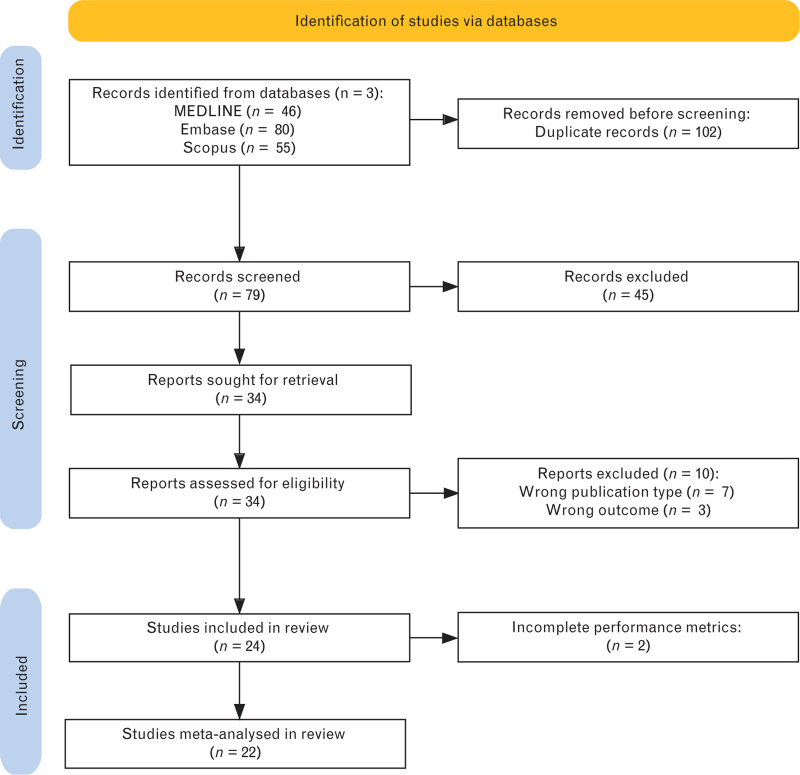
Data sources: MEDLINE, Embase and Scopus were used as data sources for relevant publications until February 2024.
Eligibility criteria: Prospective clinical studies in which the EEOT was used to predict fluid responsiveness in mechanically ventilated adults, regardless of the clinical care context. The operative performance characteristics must also have been reported.
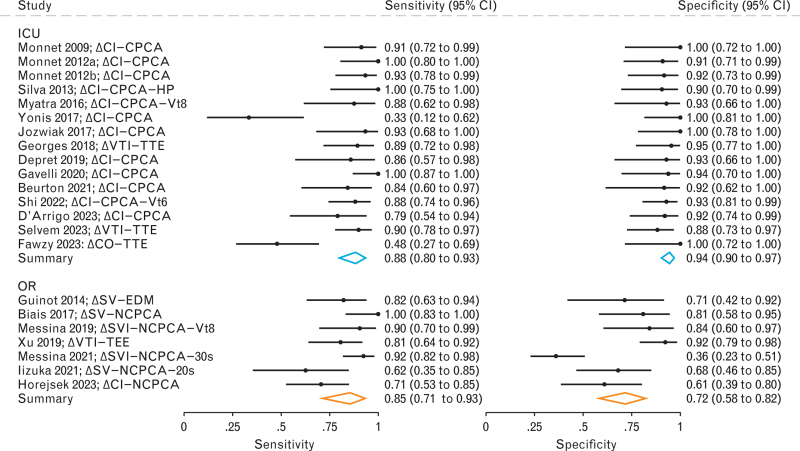
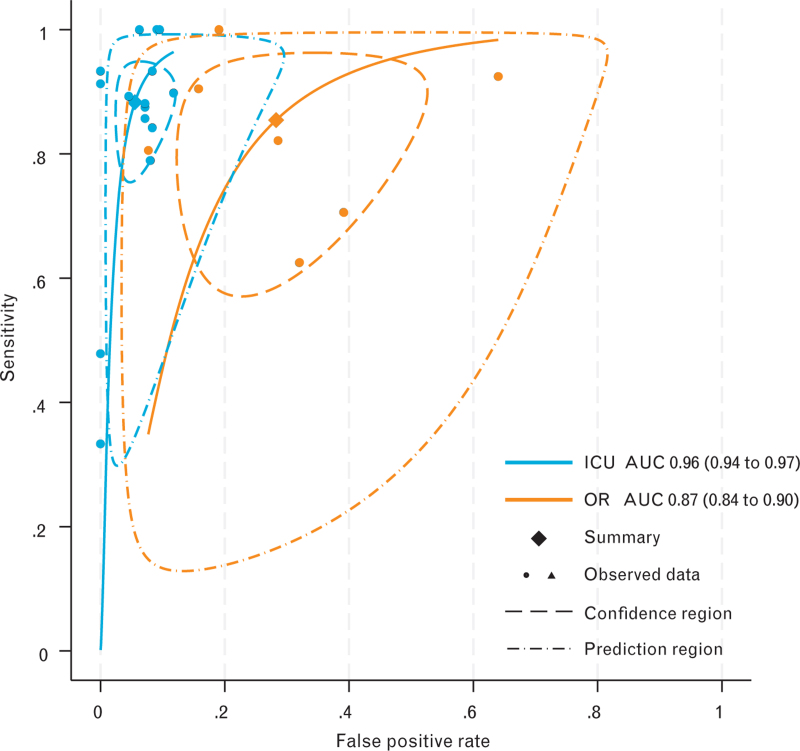
Results: Twenty-four studies involving 1073 adult patients (588 receiving intensive care and 485 in the operating room) were systematically reviewed, and 22 studies comprising 1049 volume expansions were meta-analysed. The pooled sensitivity [95% confidence interval (CI)] of the EEOT was 0.87 (0.81 to 0.92), and the pooled specificity was 0.90 (0.85 to 0.94); the median [interquartile range] cardiac index ( CI ) threshold for a positive test was a 5.0 [3.3 to 5.3] increase. The clinical context, the method used for haemodynamic monitoring, the ratio of the averaging time of the monitoring method to the occlusion time, the levels of positive end-expiratory pressure and the choice of cardiac output marker were identified as significant sources of heterogeneity. However, the occlusion duration and tidal volume did not significantly affect its performance. A novel insight is that performance was notably lower in the operating room setting. The likelihood ratios were 14 (positive) and 0.12 (negative) for the ICU, both better than 3.1 and 0.21 for the operating room. The overall quality of the evidence was assessed to be very low, mainly due to high heterogeneity and risk of bias; however, no publication bias was detected.
Conclusion: The EEOT for predicting fluid responsiveness in critical care performs acceptably well overall and is a confirmative test. In the operating room and/or with specific technical settings, its performance and clinical utility are reduced, driving the need for more context-specific and patient-specific fluid responsiveness assessments.
期刊介绍:
The European Journal of Anaesthesiology (EJA) publishes original work of high scientific quality in the field of anaesthesiology, pain, emergency medicine and intensive care. Preference is given to experimental work or clinical observation in man, and to laboratory work of clinical relevance. The journal also publishes commissioned reviews by an authority, editorials, invited commentaries, special articles, pro and con debates, and short reports (correspondences, case reports, short reports of clinical studies).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


