{"title":"一项真实世界研究:ros1阳性晚期NSCLC的治疗结果。","authors":"Hanqi Yuan, Zihua Zou, Xuezhi Hao, Yan Li, Junling Li, Jianming Ying, Puyuan Xing","doi":"10.1111/1759-7714.70086","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>ROS1 gene rearrangement is an important target for NSCLC treatment. There is not yet sufficient real-world data on ROS1 diagnostic methods, treatment selection, and clinical outcomes in the Chinese population.</p><p><strong>Methods: </strong>A single-center retrospective collection of patients with a diagnosis of ROS1-positive advanced NSCLC from July 2011 to November 2021 was performed to document the method of ROS1 testing, treatment options, efficacy, and resistance to ROS1 inhibitors in these patients.</p><p><strong>Results: </strong>The method of ROS1 testing and initial treatment selection were significantly correlated with time. ROS1 testing shifted from FISH (67% pre-2019) to NGS (96.3% post-2019; p < 0.001). First-line ROS1-TKI use increased from 60.0% to 92.0% (p = 0.041). The vast majority of patients (90.0%) chose crizotinib as the initial ROS1 inhibitor, with objective response rates (for patients with target lesions) and median progression-free survival of 82.8% (95% CI: 68.1%-97.9%) and 18.7 months (95% CI: 8.9-28.4 months), respectively. CNS was the most common site of progression for crizotinib (60%, 13/26, including 11 intracranial progressions alone). Compared to patients who received a chemotherapy-based regimen (n = 8) as first-line therapy, patients who received ROS1-TKI (n = 32) as first-line therapy had significantly longer median PFS (18.3 months vs. 3.7 months, p < 0.001). For ROS1 inhibitor-resistant patients, 48.3% of patients underwent rebiopsy throughout the course of their disease, with G2032R being the most common secondary ROS1 mutation (7/8).</p><p><strong>Conclusion: </strong>With the innovation of diagnostic and therapeutic methods and the expansion of the scope of the health insurance coverage, more and more patients are benefiting from new technologies and targeted drugs. Although crizotinib has brought excellent therapeutic data for ROS1-positive patients, better brain protection strategies should be explored for ROS1-positive patients in the future. In addition, the low rate of rebiopsy in real-world ROS1-positive patients should also be emphasized in clinical practice.</p>","PeriodicalId":23338,"journal":{"name":"Thoracic Cancer","volume":"16 9","pages":"e70086"},"PeriodicalIF":2.3000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068926/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Real-World Study: Therapeutic Outcomes of ROS1-Positive Advanced NSCLC.\",\"authors\":\"Hanqi Yuan, Zihua Zou, Xuezhi Hao, Yan Li, Junling Li, Jianming Ying, Puyuan Xing\",\"doi\":\"10.1111/1759-7714.70086\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>ROS1 gene rearrangement is an important target for NSCLC treatment. There is not yet sufficient real-world data on ROS1 diagnostic methods, treatment selection, and clinical outcomes in the Chinese population.</p><p><strong>Methods: </strong>A single-center retrospective collection of patients with a diagnosis of ROS1-positive advanced NSCLC from July 2011 to November 2021 was performed to document the method of ROS1 testing, treatment options, efficacy, and resistance to ROS1 inhibitors in these patients.</p><p><strong>Results: </strong>The method of ROS1 testing and initial treatment selection were significantly correlated with time. ROS1 testing shifted from FISH (67% pre-2019) to NGS (96.3% post-2019; p < 0.001). First-line ROS1-TKI use increased from 60.0% to 92.0% (p = 0.041). The vast majority of patients (90.0%) chose crizotinib as the initial ROS1 inhibitor, with objective response rates (for patients with target lesions) and median progression-free survival of 82.8% (95% CI: 68.1%-97.9%) and 18.7 months (95% CI: 8.9-28.4 months), respectively. CNS was the most common site of progression for crizotinib (60%, 13/26, including 11 intracranial progressions alone). Compared to patients who received a chemotherapy-based regimen (n = 8) as first-line therapy, patients who received ROS1-TKI (n = 32) as first-line therapy had significantly longer median PFS (18.3 months vs. 3.7 months, p < 0.001). For ROS1 inhibitor-resistant patients, 48.3% of patients underwent rebiopsy throughout the course of their disease, with G2032R being the most common secondary ROS1 mutation (7/8).</p><p><strong>Conclusion: </strong>With the innovation of diagnostic and therapeutic methods and the expansion of the scope of the health insurance coverage, more and more patients are benefiting from new technologies and targeted drugs. Although crizotinib has brought excellent therapeutic data for ROS1-positive patients, better brain protection strategies should be explored for ROS1-positive patients in the future. In addition, the low rate of rebiopsy in real-world ROS1-positive patients should also be emphasized in clinical practice.</p>\",\"PeriodicalId\":23338,\"journal\":{\"name\":\"Thoracic Cancer\",\"volume\":\"16 9\",\"pages\":\"e70086\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068926/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thoracic Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/1759-7714.70086\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/1759-7714.70086","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
A Real-World Study: Therapeutic Outcomes of ROS1-Positive Advanced NSCLC.
Background: ROS1 gene rearrangement is an important target for NSCLC treatment. There is not yet sufficient real-world data on ROS1 diagnostic methods, treatment selection, and clinical outcomes in the Chinese population.
Methods: A single-center retrospective collection of patients with a diagnosis of ROS1-positive advanced NSCLC from July 2011 to November 2021 was performed to document the method of ROS1 testing, treatment options, efficacy, and resistance to ROS1 inhibitors in these patients.
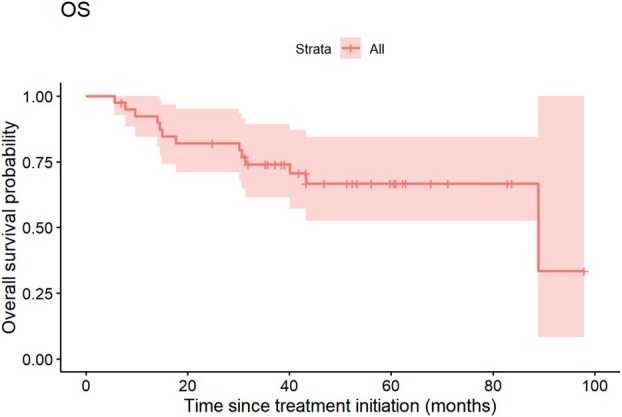
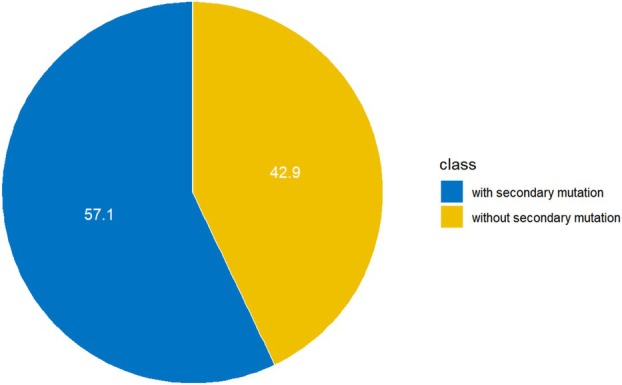
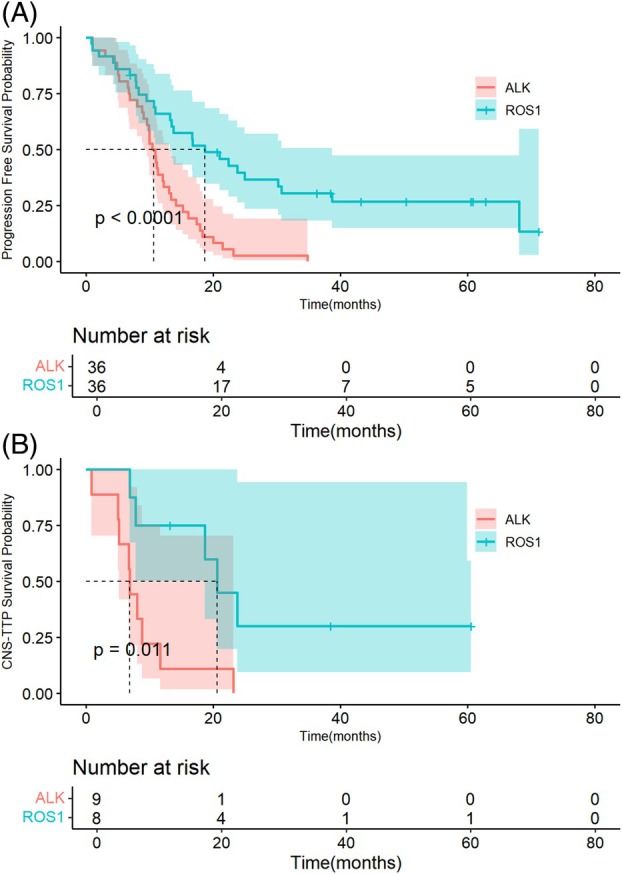
Results: The method of ROS1 testing and initial treatment selection were significantly correlated with time. ROS1 testing shifted from FISH (67% pre-2019) to NGS (96.3% post-2019; p < 0.001). First-line ROS1-TKI use increased from 60.0% to 92.0% (p = 0.041). The vast majority of patients (90.0%) chose crizotinib as the initial ROS1 inhibitor, with objective response rates (for patients with target lesions) and median progression-free survival of 82.8% (95% CI: 68.1%-97.9%) and 18.7 months (95% CI: 8.9-28.4 months), respectively. CNS was the most common site of progression for crizotinib (60%, 13/26, including 11 intracranial progressions alone). Compared to patients who received a chemotherapy-based regimen (n = 8) as first-line therapy, patients who received ROS1-TKI (n = 32) as first-line therapy had significantly longer median PFS (18.3 months vs. 3.7 months, p < 0.001). For ROS1 inhibitor-resistant patients, 48.3% of patients underwent rebiopsy throughout the course of their disease, with G2032R being the most common secondary ROS1 mutation (7/8).
Conclusion: With the innovation of diagnostic and therapeutic methods and the expansion of the scope of the health insurance coverage, more and more patients are benefiting from new technologies and targeted drugs. Although crizotinib has brought excellent therapeutic data for ROS1-positive patients, better brain protection strategies should be explored for ROS1-positive patients in the future. In addition, the low rate of rebiopsy in real-world ROS1-positive patients should also be emphasized in clinical practice.
期刊介绍:
Thoracic Cancer aims to facilitate international collaboration and exchange of comprehensive and cutting-edge information on basic, translational, and applied clinical research in lung cancer, esophageal cancer, mediastinal cancer, breast cancer and other thoracic malignancies. Prevention, treatment and research relevant to Asia-Pacific is a focus area, but submissions from all regions are welcomed. The editors encourage contributions relevant to prevention, general thoracic surgery, medical oncology, radiology, radiation medicine, pathology, basic cancer research, as well as epidemiological and translational studies in thoracic cancer. Thoracic Cancer is the official publication of the Chinese Society of Lung Cancer, International Chinese Society of Thoracic Surgery and is endorsed by the Korean Association for the Study of Lung Cancer and the Hong Kong Cancer Therapy Society.
The Journal publishes a range of article types including: Editorials, Invited Reviews, Mini Reviews, Original Articles, Clinical Guidelines, Technological Notes, Imaging in thoracic cancer, Meeting Reports, Case Reports, Letters to the Editor, Commentaries, and Brief Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


