Luigi Aurelio Nasto, Ferruccio De Prisco, Enrico Pola, Silverio Perrotta, Giuseppina Miele, Gianluca Piatelli, Claudia Santoro
{"title":"复杂NF1患儿严重颈椎后凸1例,病例报告及文献复习。","authors":"Luigi Aurelio Nasto, Ferruccio De Prisco, Enrico Pola, Silverio Perrotta, Giuseppina Miele, Gianluca Piatelli, Claudia Santoro","doi":"10.1007/s00381-025-06831-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We faced and herein report a detailed description of pre-operative assessment, management, and post-operative follow-up of a 2-year and 10-month-old girl with neurofibromatosis 1 (NF1) who presented with severe, dystrophic, cervical kyphosis (170 degrees) associated with extensive pre- and para-vertebral plexiform neurofibromas, who also went under MEK inhibitors therapy. Cervical kyphosis in NF1 is particularly rare, and there is no extensive literature available on the subject in terms of clinico-radiological features, surgical approach, and outcomes. We therefore also performed a comprehensive review of the available literature on the topic.</p><p><strong>Methods: </strong>The clinical report was made through the retrospective review of all medical documents and imaging of the patient. The systematic review was performed based on the inclusion and exclusion criteria set by the authors on surgical management of cervical kyphosis in NF1 patients according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).</p><p><strong>Results: </strong>Our patient underwent a first-stage halo-gravity traction followed by a single-stage occipito-cervical posterior fusion. The six-week traction resulted in a reduction of the deformity from 170 to 90°. A further amelioration was obtained by surgery with a final 60% correction of the curvature (69° at last post-operative X-ray). No complications were observed at 1-and-a-half-year follow-up. The plexiform neurofibromas were treated with MEK inhibitors: trametinib for 1 year and 11 months until performing halo traction, and with selumetinib after surgery. We just found 19 papers suitable according to our selection criteria.</p><p><strong>Conclusion: </strong>Combined anterior and posterior fusion (CAP) is generally the best treatment option, although it is not always feasible. When plexiform, symptomatic, inoperable neurofibromas coexist, surgery can be preceded or followed by MEK inhibitor treatment for better control or a volumetric reduction of the tumors. The best therapeutic choice should always be the result of a multidisciplinary, expert approach and patient-tailored design.</p>","PeriodicalId":9970,"journal":{"name":"Child's Nervous System","volume":"41 1","pages":"175"},"PeriodicalIF":1.2000,"publicationDate":"2025-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12065763/pdf/","citationCount":"0","resultStr":"{\"title\":\"Severe cervical kyphosis in a complex child with NF1, case report and literature review.\",\"authors\":\"Luigi Aurelio Nasto, Ferruccio De Prisco, Enrico Pola, Silverio Perrotta, Giuseppina Miele, Gianluca Piatelli, Claudia Santoro\",\"doi\":\"10.1007/s00381-025-06831-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>We faced and herein report a detailed description of pre-operative assessment, management, and post-operative follow-up of a 2-year and 10-month-old girl with neurofibromatosis 1 (NF1) who presented with severe, dystrophic, cervical kyphosis (170 degrees) associated with extensive pre- and para-vertebral plexiform neurofibromas, who also went under MEK inhibitors therapy. Cervical kyphosis in NF1 is particularly rare, and there is no extensive literature available on the subject in terms of clinico-radiological features, surgical approach, and outcomes. We therefore also performed a comprehensive review of the available literature on the topic.</p><p><strong>Methods: </strong>The clinical report was made through the retrospective review of all medical documents and imaging of the patient. The systematic review was performed based on the inclusion and exclusion criteria set by the authors on surgical management of cervical kyphosis in NF1 patients according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).</p><p><strong>Results: </strong>Our patient underwent a first-stage halo-gravity traction followed by a single-stage occipito-cervical posterior fusion. The six-week traction resulted in a reduction of the deformity from 170 to 90°. A further amelioration was obtained by surgery with a final 60% correction of the curvature (69° at last post-operative X-ray). No complications were observed at 1-and-a-half-year follow-up. The plexiform neurofibromas were treated with MEK inhibitors: trametinib for 1 year and 11 months until performing halo traction, and with selumetinib after surgery. We just found 19 papers suitable according to our selection criteria.</p><p><strong>Conclusion: </strong>Combined anterior and posterior fusion (CAP) is generally the best treatment option, although it is not always feasible. When plexiform, symptomatic, inoperable neurofibromas coexist, surgery can be preceded or followed by MEK inhibitor treatment for better control or a volumetric reduction of the tumors. The best therapeutic choice should always be the result of a multidisciplinary, expert approach and patient-tailored design.</p>\",\"PeriodicalId\":9970,\"journal\":{\"name\":\"Child's Nervous System\",\"volume\":\"41 1\",\"pages\":\"175\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-05-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12065763/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Child's Nervous System\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00381-025-06831-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Child's Nervous System","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00381-025-06831-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Severe cervical kyphosis in a complex child with NF1, case report and literature review.
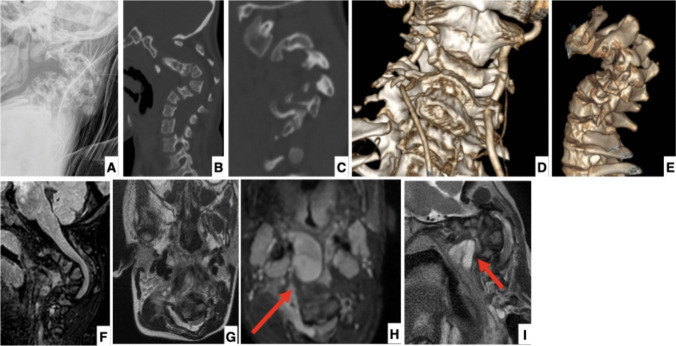
Purpose: We faced and herein report a detailed description of pre-operative assessment, management, and post-operative follow-up of a 2-year and 10-month-old girl with neurofibromatosis 1 (NF1) who presented with severe, dystrophic, cervical kyphosis (170 degrees) associated with extensive pre- and para-vertebral plexiform neurofibromas, who also went under MEK inhibitors therapy. Cervical kyphosis in NF1 is particularly rare, and there is no extensive literature available on the subject in terms of clinico-radiological features, surgical approach, and outcomes. We therefore also performed a comprehensive review of the available literature on the topic.
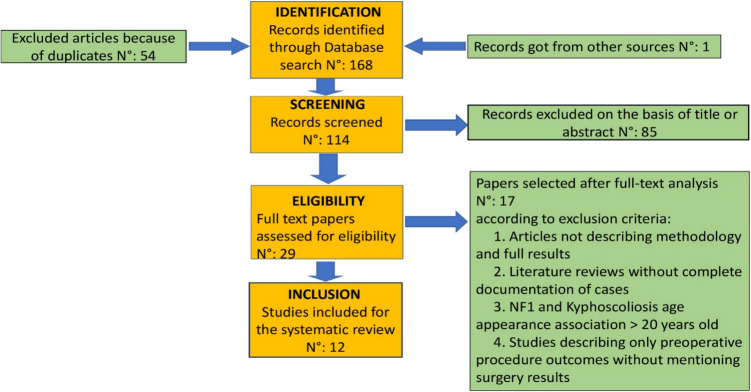
Methods: The clinical report was made through the retrospective review of all medical documents and imaging of the patient. The systematic review was performed based on the inclusion and exclusion criteria set by the authors on surgical management of cervical kyphosis in NF1 patients according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
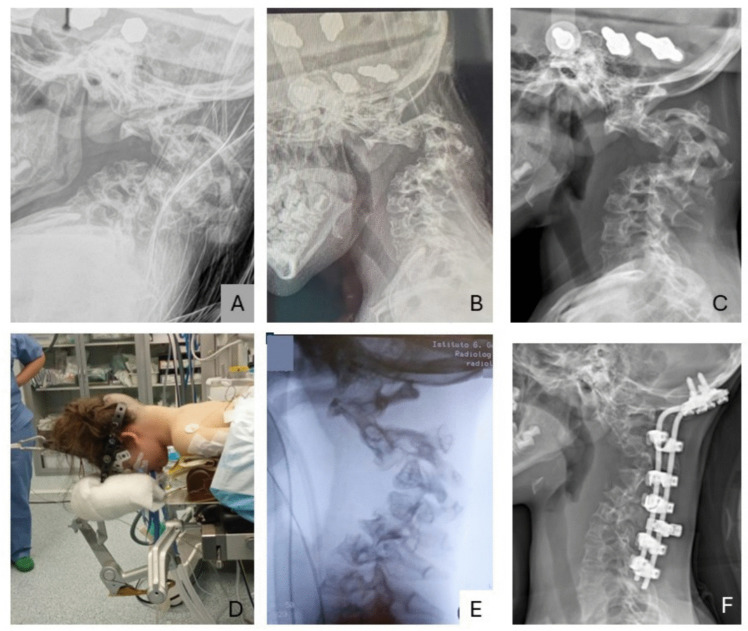
Results: Our patient underwent a first-stage halo-gravity traction followed by a single-stage occipito-cervical posterior fusion. The six-week traction resulted in a reduction of the deformity from 170 to 90°. A further amelioration was obtained by surgery with a final 60% correction of the curvature (69° at last post-operative X-ray). No complications were observed at 1-and-a-half-year follow-up. The plexiform neurofibromas were treated with MEK inhibitors: trametinib for 1 year and 11 months until performing halo traction, and with selumetinib after surgery. We just found 19 papers suitable according to our selection criteria.
Conclusion: Combined anterior and posterior fusion (CAP) is generally the best treatment option, although it is not always feasible. When plexiform, symptomatic, inoperable neurofibromas coexist, surgery can be preceded or followed by MEK inhibitor treatment for better control or a volumetric reduction of the tumors. The best therapeutic choice should always be the result of a multidisciplinary, expert approach and patient-tailored design.
期刊介绍:
The journal has been expanded to encompass all aspects of pediatric neurosciences concerning the developmental and acquired abnormalities of the nervous system and its coverings, functional disorders, epilepsy, spasticity, basic and clinical neuro-oncology, rehabilitation and trauma. Global pediatric neurosurgery is an additional field of interest that will be considered for publication in the journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


