{"title":"血浆糖胺聚糖作为生物标志物改善肺癌风险分层的外部验证。","authors":"Michael P A Davies, John K Field, Francesco Gatto","doi":"10.1158/1055-9965.EPI-24-1537","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung cancer screening excludes individuals not considered at an increased risk for lung cancer, as predicted by risk models like the Liverpool Lung Project version 3 (LLPv3). In this study, we sought to validate whether plasma glycosaminoglycan profiles (GAGomes) could predict lung cancer independent of LLPv3 and other prespecified comorbidities.</p><p><strong>Methods: </strong>In this retrospective cohort-based case-control study, we included patients who were suspected of having lung cancer at baseline and were either diagnosed with lung cancer (cases) or remained cancer-free for 5 years after baseline (controls). Plasma GAGomes were measured at baseline and used to compute a prespecified GAGome score to discriminate lung cancer from controls. We then applied multivariable Bayesian logistic regression to evaluate the likelihood that 7 LLPv3 predictors or 14 comorbidities had an effect on the GAGome score. We tested the independence of the GAGome score from LLPv3-predicted 5-year risk using the likelihood ratio test and assessed whether it improved lung cancer risk prediction in a set equivalent to an LLPv3-predicted 5-year risk of ≥1.51%.</p><p><strong>Results: </strong>We included 653 lung cancer and 653 controls. The AUC of the GAGome score was 0.63 (95% confidence interval, 0.62-63). None of the LLPv3 predictors or comorbidities were compatible with a significant effect on the score. The GAGome score was independent of LLPv3 (P < 0.001) and improved its sensitivity (72% vs. 69%) and specificity (61% vs. 59%).</p><p><strong>Conclusions: </strong>Plasma GAGomes identified additional lung cancer cases beyond those predicted by LLPv3 alone.</p><p><strong>Impact: </strong>GAGomes could improve risk-stratified lung cancer if validated in a screening population.</p>","PeriodicalId":9458,"journal":{"name":"Cancer Epidemiology Biomarkers & Prevention","volume":" ","pages":"1219-1225"},"PeriodicalIF":3.4000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12209813/pdf/","citationCount":"0","resultStr":"{\"title\":\"External Validation of Plasma Glycosaminoglycans as Biomarkers to Improve Lung Cancer Risk Stratification.\",\"authors\":\"Michael P A Davies, John K Field, Francesco Gatto\",\"doi\":\"10.1158/1055-9965.EPI-24-1537\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Lung cancer screening excludes individuals not considered at an increased risk for lung cancer, as predicted by risk models like the Liverpool Lung Project version 3 (LLPv3). In this study, we sought to validate whether plasma glycosaminoglycan profiles (GAGomes) could predict lung cancer independent of LLPv3 and other prespecified comorbidities.</p><p><strong>Methods: </strong>In this retrospective cohort-based case-control study, we included patients who were suspected of having lung cancer at baseline and were either diagnosed with lung cancer (cases) or remained cancer-free for 5 years after baseline (controls). Plasma GAGomes were measured at baseline and used to compute a prespecified GAGome score to discriminate lung cancer from controls. We then applied multivariable Bayesian logistic regression to evaluate the likelihood that 7 LLPv3 predictors or 14 comorbidities had an effect on the GAGome score. We tested the independence of the GAGome score from LLPv3-predicted 5-year risk using the likelihood ratio test and assessed whether it improved lung cancer risk prediction in a set equivalent to an LLPv3-predicted 5-year risk of ≥1.51%.</p><p><strong>Results: </strong>We included 653 lung cancer and 653 controls. The AUC of the GAGome score was 0.63 (95% confidence interval, 0.62-63). None of the LLPv3 predictors or comorbidities were compatible with a significant effect on the score. The GAGome score was independent of LLPv3 (P < 0.001) and improved its sensitivity (72% vs. 69%) and specificity (61% vs. 59%).</p><p><strong>Conclusions: </strong>Plasma GAGomes identified additional lung cancer cases beyond those predicted by LLPv3 alone.</p><p><strong>Impact: </strong>GAGomes could improve risk-stratified lung cancer if validated in a screening population.</p>\",\"PeriodicalId\":9458,\"journal\":{\"name\":\"Cancer Epidemiology Biomarkers & Prevention\",\"volume\":\" \",\"pages\":\"1219-1225\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12209813/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Epidemiology Biomarkers & Prevention\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1158/1055-9965.EPI-24-1537\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Epidemiology Biomarkers & Prevention","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1158/1055-9965.EPI-24-1537","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:肺癌(LC)筛查排除了像利物浦肺项目第3版(LLPv3)这样的风险模型所预测的没有增加肺癌风险的个体。在这里,我们试图验证血浆糖胺聚糖谱(GAGomes)是否可以独立于LLPv3和其他预先指定的合病预测LC。方法:在这项基于队列的回顾性病例对照研究中,我们纳入了基线时怀疑患有LC的患者,这些患者要么被诊断患有LC(病例),要么在基线后5年内没有癌症(对照组)。在基线时测量血浆GAGome,并用于计算预先指定的GAGome评分,以区分LC和对照组。然后,我们应用多变量贝叶斯逻辑回归来评估7种LLPv3预测因子或14种合并症对GAGome评分影响的可能性。我们使用似然比检验检验了GAGome评分与llpv3预测的5年风险的独立性,并评估了它是否改善了llpv3预测的5年风险≥1.51%的LC风险预测。结果:纳入653例LC和653例对照。GAGome评分的AUC为0.63 (95% CI = 0.62-63)。没有一个LLPv3预测因子或合并症对评分有显著影响。GAGome评分独立于LLPv3 (p < 0.001),提高了其敏感性(72%对69%)和特异性(61%对59%)。结论:血浆GAGomes检测到的LC病例比单独使用LLPv3预测的要多。影响:如果在筛查人群中得到验证,GAGomes可以改善风险分层的LC。
External Validation of Plasma Glycosaminoglycans as Biomarkers to Improve Lung Cancer Risk Stratification.
Background: Lung cancer screening excludes individuals not considered at an increased risk for lung cancer, as predicted by risk models like the Liverpool Lung Project version 3 (LLPv3). In this study, we sought to validate whether plasma glycosaminoglycan profiles (GAGomes) could predict lung cancer independent of LLPv3 and other prespecified comorbidities.
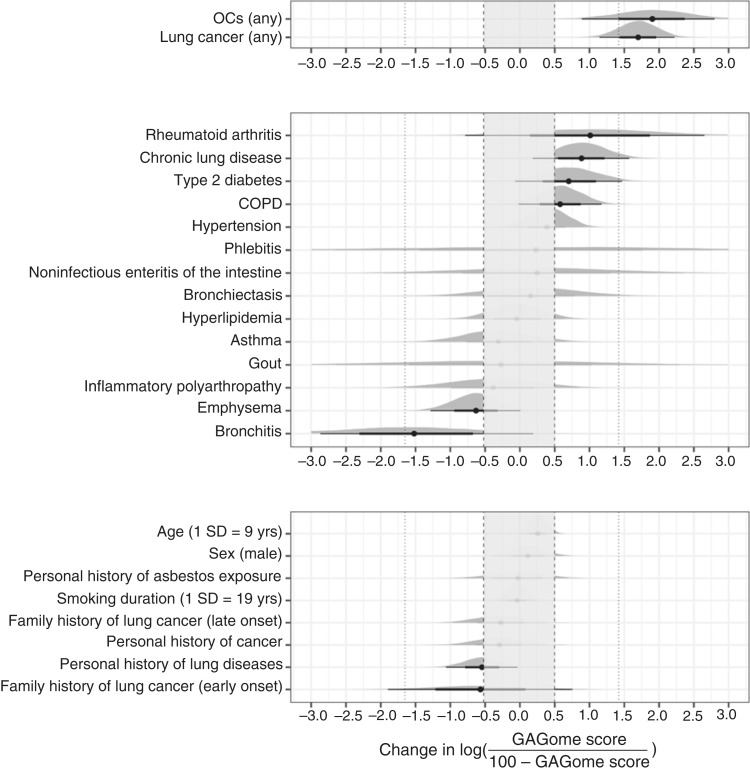
Methods: In this retrospective cohort-based case-control study, we included patients who were suspected of having lung cancer at baseline and were either diagnosed with lung cancer (cases) or remained cancer-free for 5 years after baseline (controls). Plasma GAGomes were measured at baseline and used to compute a prespecified GAGome score to discriminate lung cancer from controls. We then applied multivariable Bayesian logistic regression to evaluate the likelihood that 7 LLPv3 predictors or 14 comorbidities had an effect on the GAGome score. We tested the independence of the GAGome score from LLPv3-predicted 5-year risk using the likelihood ratio test and assessed whether it improved lung cancer risk prediction in a set equivalent to an LLPv3-predicted 5-year risk of ≥1.51%.
Results: We included 653 lung cancer and 653 controls. The AUC of the GAGome score was 0.63 (95% confidence interval, 0.62-63). None of the LLPv3 predictors or comorbidities were compatible with a significant effect on the score. The GAGome score was independent of LLPv3 (P < 0.001) and improved its sensitivity (72% vs. 69%) and specificity (61% vs. 59%).
Conclusions: Plasma GAGomes identified additional lung cancer cases beyond those predicted by LLPv3 alone.
Impact: GAGomes could improve risk-stratified lung cancer if validated in a screening population.
期刊介绍:
Cancer Epidemiology, Biomarkers & Prevention publishes original peer-reviewed, population-based research on cancer etiology, prevention, surveillance, and survivorship. The following topics are of special interest: descriptive, analytical, and molecular epidemiology; biomarkers including assay development, validation, and application; chemoprevention and other types of prevention research in the context of descriptive and observational studies; the role of behavioral factors in cancer etiology and prevention; survivorship studies; risk factors; implementation science and cancer care delivery; and the science of cancer health disparities. Besides welcoming manuscripts that address individual subjects in any of the relevant disciplines, CEBP editors encourage the submission of manuscripts with a transdisciplinary approach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


