{"title":"偏倚抗体及其他:甲状旁腺激素依赖性高钙血症诊断的新时代。","authors":"Noriko Makita, Katsunori Manaka, Maho Taguchi, Hirofumi Horikoshi, Junichiro Sato, Taroh Iiri","doi":"10.1507/endocrj.EJ25-0051","DOIUrl":null,"url":null,"abstract":"<p><p>Hypercalcemia, a common electrolyte imbalance, requires accurate differential diagnosis to guide appropriate management. PTH-dependent hypercalcemia, predominantly caused by primary hyperparathyroidism (PHPT) and rarely by familial hypocalciuric hypercalcemia (FHH)-mainly due to heterozygous loss-of-function mutations in the CASR gene encoding the calcium-sensing receptor (CaSR)-now includes acquired hypocalciuric hypercalcemia (AHH) as an emerging disease entity. Initially identified as analogous to FHH, AHH was characterized by blocking antibodies targeting the CaSR. However, our research has identified unique autoantibodies, termed biased antibodies, that paradoxically regulate signaling by enhancing Gq activity while suppressing Gi activity. Investigating their mechanisms has not only provided insights into specific treatments for AHH but also suggested novel activation mechanisms and binding sites of the CaSR, offering a fresh perspective on the regulation of PTH secretion. In clinical practice, recognizing AHH is crucial. A key diagnostic feature is fluctuating serum calcium levels, making a wait-and-see approach viable for mild hypercalcemia. Conversely, hypercalcemic crises necessitate immediate diagnostic and therapeutic interventions. The most important diagnostic clue to differentiate AHH from PHPT is hypermagnesemia. Additionally, AHH is less likely to involve AVP resistance (i.e., nephrogenic diabetes insipidus) and acute kidney injury (AKI), owing to preserved medullary hyperosmolarity and minimal interference with AVP signaling. Finally, a relatively low PTH level serves as another distinguishing feature. Based on these observations, we propose a novel diagnostic guide for PTH-dependent hypercalcemia. We anticipate that this guide will help identify previously undiagnosed AHH cases in routine practice, enabling timely and effective management of this rare condition.</p>","PeriodicalId":11631,"journal":{"name":"Endocrine journal","volume":" ","pages":"967-978"},"PeriodicalIF":2.1000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436076/pdf/","citationCount":"0","resultStr":"{\"title\":\"Biased antibodies and beyond: a new era in the diagnosis of PTH-dependent hypercalcemia.\",\"authors\":\"Noriko Makita, Katsunori Manaka, Maho Taguchi, Hirofumi Horikoshi, Junichiro Sato, Taroh Iiri\",\"doi\":\"10.1507/endocrj.EJ25-0051\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Hypercalcemia, a common electrolyte imbalance, requires accurate differential diagnosis to guide appropriate management. PTH-dependent hypercalcemia, predominantly caused by primary hyperparathyroidism (PHPT) and rarely by familial hypocalciuric hypercalcemia (FHH)-mainly due to heterozygous loss-of-function mutations in the CASR gene encoding the calcium-sensing receptor (CaSR)-now includes acquired hypocalciuric hypercalcemia (AHH) as an emerging disease entity. Initially identified as analogous to FHH, AHH was characterized by blocking antibodies targeting the CaSR. However, our research has identified unique autoantibodies, termed biased antibodies, that paradoxically regulate signaling by enhancing Gq activity while suppressing Gi activity. Investigating their mechanisms has not only provided insights into specific treatments for AHH but also suggested novel activation mechanisms and binding sites of the CaSR, offering a fresh perspective on the regulation of PTH secretion. In clinical practice, recognizing AHH is crucial. A key diagnostic feature is fluctuating serum calcium levels, making a wait-and-see approach viable for mild hypercalcemia. Conversely, hypercalcemic crises necessitate immediate diagnostic and therapeutic interventions. The most important diagnostic clue to differentiate AHH from PHPT is hypermagnesemia. Additionally, AHH is less likely to involve AVP resistance (i.e., nephrogenic diabetes insipidus) and acute kidney injury (AKI), owing to preserved medullary hyperosmolarity and minimal interference with AVP signaling. Finally, a relatively low PTH level serves as another distinguishing feature. Based on these observations, we propose a novel diagnostic guide for PTH-dependent hypercalcemia. We anticipate that this guide will help identify previously undiagnosed AHH cases in routine practice, enabling timely and effective management of this rare condition.</p>\",\"PeriodicalId\":11631,\"journal\":{\"name\":\"Endocrine journal\",\"volume\":\" \",\"pages\":\"967-978\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436076/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1507/endocrj.EJ25-0051\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1507/endocrj.EJ25-0051","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/3 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Biased antibodies and beyond: a new era in the diagnosis of PTH-dependent hypercalcemia.
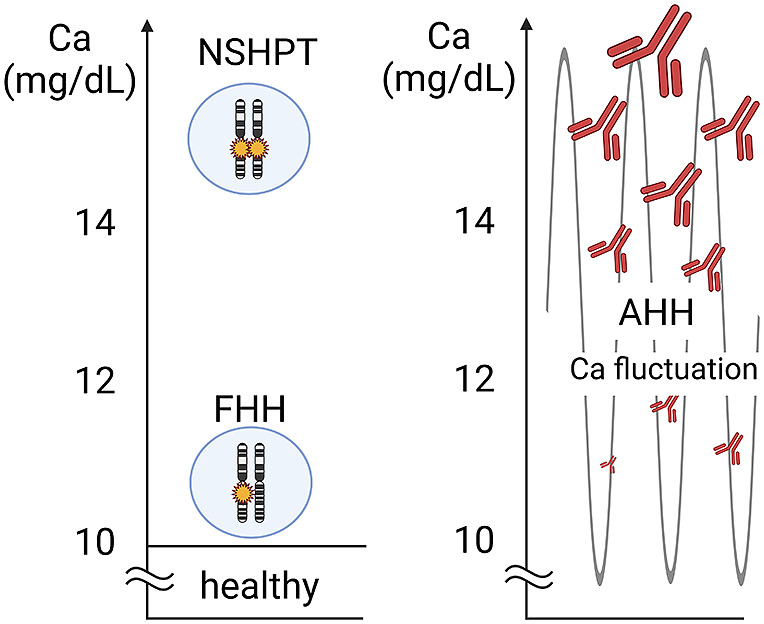
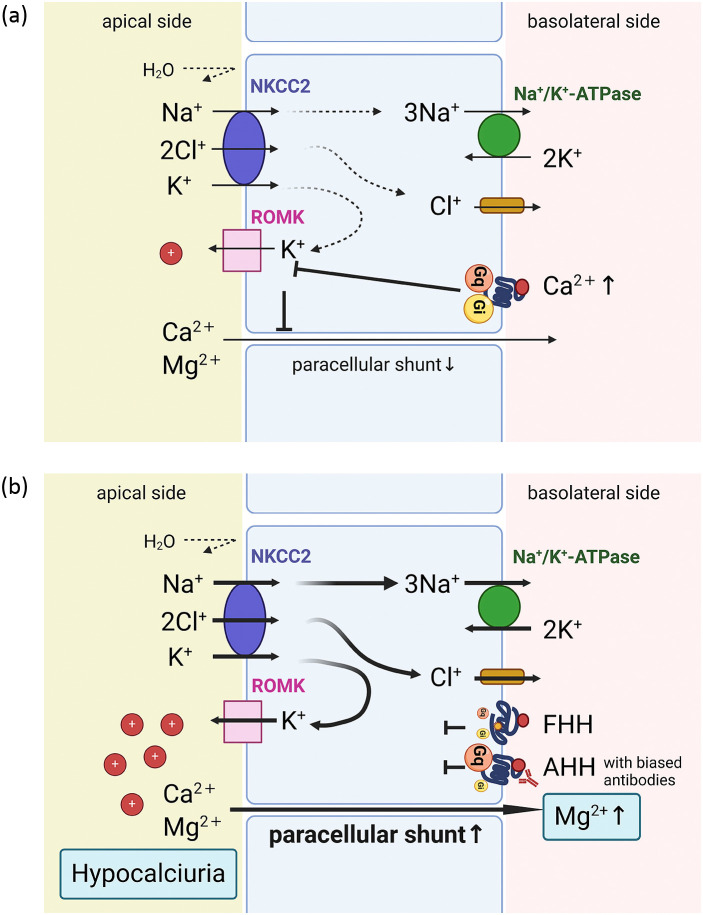
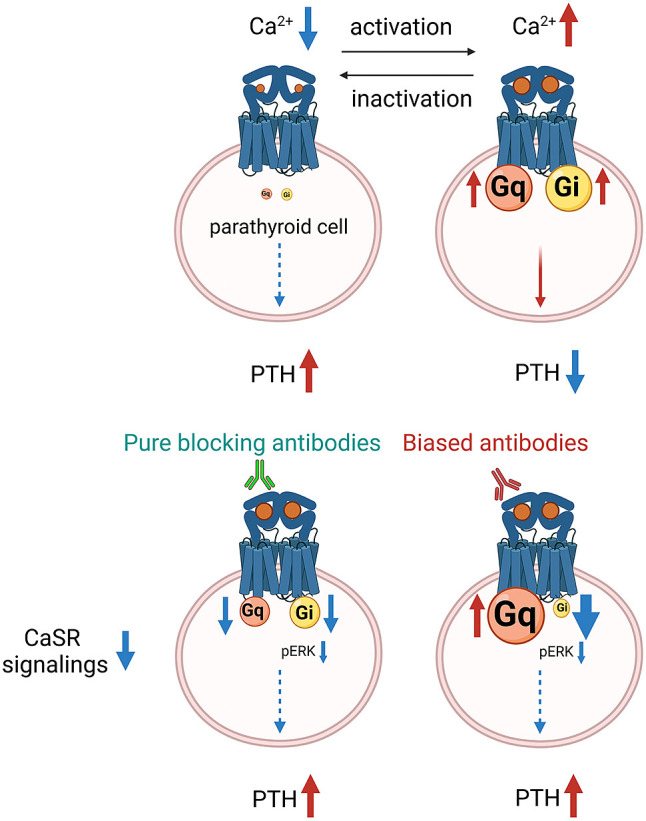
Hypercalcemia, a common electrolyte imbalance, requires accurate differential diagnosis to guide appropriate management. PTH-dependent hypercalcemia, predominantly caused by primary hyperparathyroidism (PHPT) and rarely by familial hypocalciuric hypercalcemia (FHH)-mainly due to heterozygous loss-of-function mutations in the CASR gene encoding the calcium-sensing receptor (CaSR)-now includes acquired hypocalciuric hypercalcemia (AHH) as an emerging disease entity. Initially identified as analogous to FHH, AHH was characterized by blocking antibodies targeting the CaSR. However, our research has identified unique autoantibodies, termed biased antibodies, that paradoxically regulate signaling by enhancing Gq activity while suppressing Gi activity. Investigating their mechanisms has not only provided insights into specific treatments for AHH but also suggested novel activation mechanisms and binding sites of the CaSR, offering a fresh perspective on the regulation of PTH secretion. In clinical practice, recognizing AHH is crucial. A key diagnostic feature is fluctuating serum calcium levels, making a wait-and-see approach viable for mild hypercalcemia. Conversely, hypercalcemic crises necessitate immediate diagnostic and therapeutic interventions. The most important diagnostic clue to differentiate AHH from PHPT is hypermagnesemia. Additionally, AHH is less likely to involve AVP resistance (i.e., nephrogenic diabetes insipidus) and acute kidney injury (AKI), owing to preserved medullary hyperosmolarity and minimal interference with AVP signaling. Finally, a relatively low PTH level serves as another distinguishing feature. Based on these observations, we propose a novel diagnostic guide for PTH-dependent hypercalcemia. We anticipate that this guide will help identify previously undiagnosed AHH cases in routine practice, enabling timely and effective management of this rare condition.
期刊介绍:
Endocrine Journal is an open access, peer-reviewed online journal with a long history. This journal publishes peer-reviewed research articles in multifaceted fields of basic, translational and clinical endocrinology. Endocrine Journal provides a chance to exchange your ideas, concepts and scientific observations in any area of recent endocrinology. Manuscripts may be submitted as Original Articles, Notes, Rapid Communications or Review Articles. We have a rapid reviewing and editorial decision system and pay a special attention to our quick, truly scientific and frequently-citable publication. Please go through the link for author guideline.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


