Dilaram Acharya, Tayler D Scory, Nusrat Shommu, Maoliosa Donald, Tyrone G Harrison, Jonathan S Murray, Simon Sawhney, Edward D Siew, Neesh Pannu, Matthew T James
{"title":"肾科医生对严重慢性肾病风险的认知和急性肾损伤住院后的门诊随访:多国随机调查研究。","authors":"Dilaram Acharya, Tayler D Scory, Nusrat Shommu, Maoliosa Donald, Tyrone G Harrison, Jonathan S Murray, Simon Sawhney, Edward D Siew, Neesh Pannu, Matthew T James","doi":"10.1177/20543581251336548","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients hospitalized with acute kidney injury (AKI) have variable risks for chronic kidney disease (CKD); however, there is limited knowledge about how this risk influences outpatient follow-up with nephrologists.</p><p><strong>Objective: </strong>This survey study examined the likelihood that nephrologists would recommend outpatient follow-up of patients with varying risk profiles for CKD after hospitalization with AKI and the effect of reporting the predicted risk of severe CKD on their decision-making.</p><p><strong>Design: </strong>A randomized survey study examining the impact of providing predicted risks of severe CKD on nephrologists' follow-up recommendations for patients with AKI.</p><p><strong>Setting: </strong>The study included nephrologists from the United States, the United Kingdom, and Canada between September and December 2023.</p><p><strong>Patients: </strong>Participants reviewed clinical vignettes of patients with AKI and varying risks of severe CKD (G4 or G5), using an externally validated prediction model.</p><p><strong>Measurements: </strong>The primary outcome was the likelihood of recommending nephrologist specialist follow-up for each case, scored on a 7-point Likert scale (1 = \"definitely not\" and 7 = \"definitely would\").</p><p><strong>Methods: </strong>Participants were randomized to receive a version of the survey either with or without the predicted risk of severe CKD included for each vignette. Responses were compared across categories of predicted risk (<10%, 10%-49%, and ≥50%) using generalized estimating equations.</p><p><strong>Results: </strong>Of the 203 nephrologists who participated, 73 (36%) were from the United Kingdom, 71 (35%) from Canada, and 45 (22%) from the United States. Mean (95% confidence interval [CI]) Likert scores increased from 4.01 (3.68, 4.34) for patients with a <10% predicted risk to 6.06 (5.76, 6.37) for those with a ≥ 50% predicted risk of severe CKD. Nephrologists were significantly less likely to recommend outpatient nephrology follow-up for patients with a <10% predicted risk of severe CKD when the risk was reported (mean difference = -0.71 [95% CI = -1.19, -0.23]), and significantly more likely to recommend follow-up for patients with a ≥50% predicted risk when the risk of severe CKD was reported (mean difference = 0.49 [95% CI = 0.04, 0.93]).</p><p><strong>Limitations: </strong>This study focuses on nephrologists from high-income countries and relies on hypothetical scenarios rather than real-world practices. Survey respondents may not be representative of all nephrologists, although consistent findings across diverse subgroups strengthen findings.</p><p><strong>Conclusions: </strong>When the predicted risk of severe CKD is reported, nephrologists are less likely to recommend follow-up for lower risk patients with AKI and more likely to recommend follow-up for higher risk patients, leading to better alignment of recommendations for outpatient follow-up with patient risk of severe CKD.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251336548"},"PeriodicalIF":1.5000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12046161/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nephrologist's Perceptions of Risk of Severe Chronic Kidney Disease and Outpatient Follow-up After Hospitalization With AKI: Multinational Randomized Survey Study.\",\"authors\":\"Dilaram Acharya, Tayler D Scory, Nusrat Shommu, Maoliosa Donald, Tyrone G Harrison, Jonathan S Murray, Simon Sawhney, Edward D Siew, Neesh Pannu, Matthew T James\",\"doi\":\"10.1177/20543581251336548\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients hospitalized with acute kidney injury (AKI) have variable risks for chronic kidney disease (CKD); however, there is limited knowledge about how this risk influences outpatient follow-up with nephrologists.</p><p><strong>Objective: </strong>This survey study examined the likelihood that nephrologists would recommend outpatient follow-up of patients with varying risk profiles for CKD after hospitalization with AKI and the effect of reporting the predicted risk of severe CKD on their decision-making.</p><p><strong>Design: </strong>A randomized survey study examining the impact of providing predicted risks of severe CKD on nephrologists' follow-up recommendations for patients with AKI.</p><p><strong>Setting: </strong>The study included nephrologists from the United States, the United Kingdom, and Canada between September and December 2023.</p><p><strong>Patients: </strong>Participants reviewed clinical vignettes of patients with AKI and varying risks of severe CKD (G4 or G5), using an externally validated prediction model.</p><p><strong>Measurements: </strong>The primary outcome was the likelihood of recommending nephrologist specialist follow-up for each case, scored on a 7-point Likert scale (1 = \\\"definitely not\\\" and 7 = \\\"definitely would\\\").</p><p><strong>Methods: </strong>Participants were randomized to receive a version of the survey either with or without the predicted risk of severe CKD included for each vignette. Responses were compared across categories of predicted risk (<10%, 10%-49%, and ≥50%) using generalized estimating equations.</p><p><strong>Results: </strong>Of the 203 nephrologists who participated, 73 (36%) were from the United Kingdom, 71 (35%) from Canada, and 45 (22%) from the United States. Mean (95% confidence interval [CI]) Likert scores increased from 4.01 (3.68, 4.34) for patients with a <10% predicted risk to 6.06 (5.76, 6.37) for those with a ≥ 50% predicted risk of severe CKD. Nephrologists were significantly less likely to recommend outpatient nephrology follow-up for patients with a <10% predicted risk of severe CKD when the risk was reported (mean difference = -0.71 [95% CI = -1.19, -0.23]), and significantly more likely to recommend follow-up for patients with a ≥50% predicted risk when the risk of severe CKD was reported (mean difference = 0.49 [95% CI = 0.04, 0.93]).</p><p><strong>Limitations: </strong>This study focuses on nephrologists from high-income countries and relies on hypothetical scenarios rather than real-world practices. Survey respondents may not be representative of all nephrologists, although consistent findings across diverse subgroups strengthen findings.</p><p><strong>Conclusions: </strong>When the predicted risk of severe CKD is reported, nephrologists are less likely to recommend follow-up for lower risk patients with AKI and more likely to recommend follow-up for higher risk patients, leading to better alignment of recommendations for outpatient follow-up with patient risk of severe CKD.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"12 \",\"pages\":\"20543581251336548\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12046161/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581251336548\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251336548","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Nephrologist's Perceptions of Risk of Severe Chronic Kidney Disease and Outpatient Follow-up After Hospitalization With AKI: Multinational Randomized Survey Study.
Background: Patients hospitalized with acute kidney injury (AKI) have variable risks for chronic kidney disease (CKD); however, there is limited knowledge about how this risk influences outpatient follow-up with nephrologists.
Objective: This survey study examined the likelihood that nephrologists would recommend outpatient follow-up of patients with varying risk profiles for CKD after hospitalization with AKI and the effect of reporting the predicted risk of severe CKD on their decision-making.
Design: A randomized survey study examining the impact of providing predicted risks of severe CKD on nephrologists' follow-up recommendations for patients with AKI.
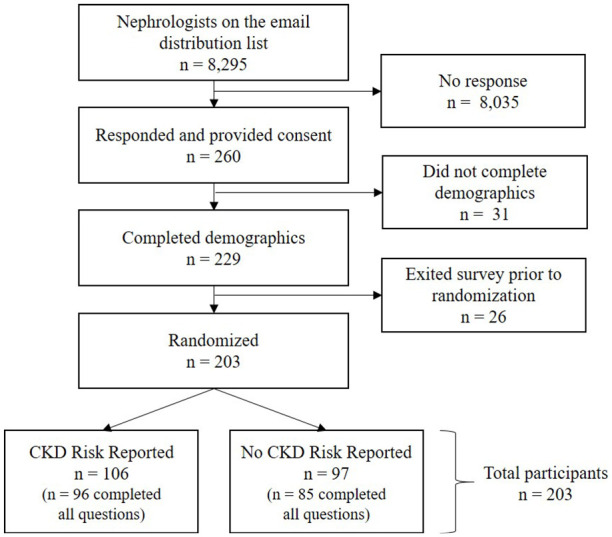
Setting: The study included nephrologists from the United States, the United Kingdom, and Canada between September and December 2023.
Patients: Participants reviewed clinical vignettes of patients with AKI and varying risks of severe CKD (G4 or G5), using an externally validated prediction model.
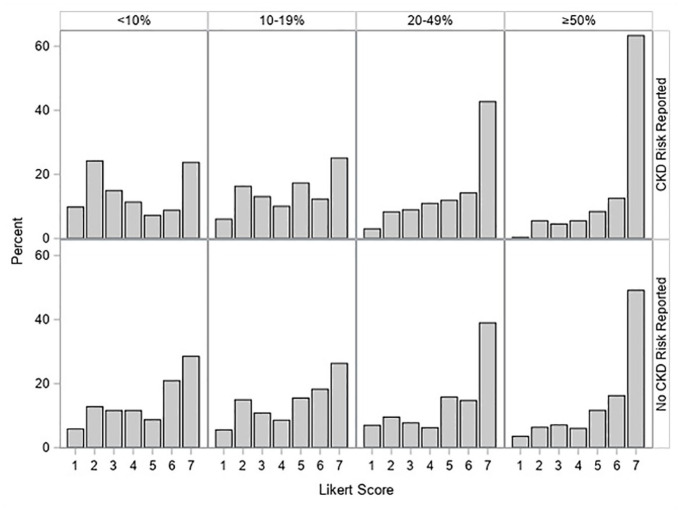
Measurements: The primary outcome was the likelihood of recommending nephrologist specialist follow-up for each case, scored on a 7-point Likert scale (1 = "definitely not" and 7 = "definitely would").
Methods: Participants were randomized to receive a version of the survey either with or without the predicted risk of severe CKD included for each vignette. Responses were compared across categories of predicted risk (<10%, 10%-49%, and ≥50%) using generalized estimating equations.
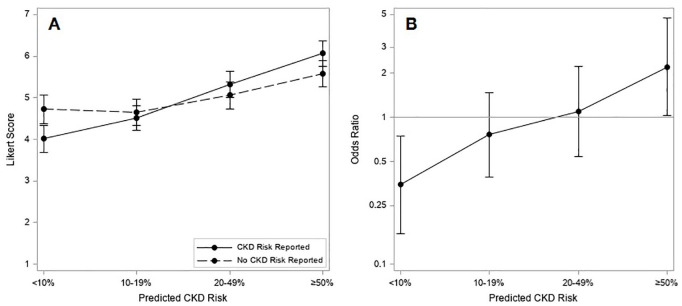
Results: Of the 203 nephrologists who participated, 73 (36%) were from the United Kingdom, 71 (35%) from Canada, and 45 (22%) from the United States. Mean (95% confidence interval [CI]) Likert scores increased from 4.01 (3.68, 4.34) for patients with a <10% predicted risk to 6.06 (5.76, 6.37) for those with a ≥ 50% predicted risk of severe CKD. Nephrologists were significantly less likely to recommend outpatient nephrology follow-up for patients with a <10% predicted risk of severe CKD when the risk was reported (mean difference = -0.71 [95% CI = -1.19, -0.23]), and significantly more likely to recommend follow-up for patients with a ≥50% predicted risk when the risk of severe CKD was reported (mean difference = 0.49 [95% CI = 0.04, 0.93]).
Limitations: This study focuses on nephrologists from high-income countries and relies on hypothetical scenarios rather than real-world practices. Survey respondents may not be representative of all nephrologists, although consistent findings across diverse subgroups strengthen findings.
Conclusions: When the predicted risk of severe CKD is reported, nephrologists are less likely to recommend follow-up for lower risk patients with AKI and more likely to recommend follow-up for higher risk patients, leading to better alignment of recommendations for outpatient follow-up with patient risk of severe CKD.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


