{"title":"强烈慢性炎症引起的严重退行性变所致的异常结节性甲状腺肿伴喉返神经麻痹1例,附组织病理学证据及文献复习。","authors":"Ryo Takagi, Kosei Mori, Sayumi Tsuyuguchi, Takashi Koike, Dinh Nam Nguyen, Kengo Kanai, Yoshihiro Watanabe, Mitsuhiro Okano, Yoshihiro Noguchi, Yuichiro Hayashi, Yorihisa Imanishi","doi":"10.1186/s12902-025-01929-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Thyroid tumors presenting with recurrent laryngeal nerve (RLN) palsy are generally considered malignant; however, RLN palsy has been reported even in benign thyroid disease (BTD), mainly due to compression or stretching, although seemingly quite rare. Herein, we report an unusual case of nodular goiter that was extremely difficult to differentiate preoperatively from thyroid malignancy because of the concomitant ipsilateral RLN palsy caused by chronic inflammation.</p><p><strong>Case presentation: </strong>A 59-year-old Japanese female presented with hoarseness and pharyngeal discomfort. Endoscopic examination revealed fixation of the right vocal cord, presumably due to right RLN palsy. Ultrasonography and computed tomography showed an ill-defined thyroid mass lesion in the right lobe, strongly suggestive of malignancy, although repeated aspiration cytology revealed no suspicion of malignancy. Intraoperatively, because the right RLN was found to be entirely embedded within the hard mass lesion and completely unresponsive to nerve integrity monitoring, the nerve was unavoidably excised along with the right lobe. Histopathology led to the final diagnosis of nodular goiter, wherein the resected RLN was severely degenerated and disrupted due to intense chronic inflammation accompanied by perineural fibrosis.</p><p><strong>Conclusions: </strong>Our literature review suggests that RLN palsy associated with thyroid mass lesions should not be considered a definitive indicator of malignancy because it can also be observed in BTD, although it is significantly less frequent than in malignancy as corroborated by our meta-analysis. Even in BTD, if the primary cause of the coexisting RLN palsy is severe chronic inflammation, nerve preservation is potentially unfeasible.</p>","PeriodicalId":9152,"journal":{"name":"BMC Endocrine Disorders","volume":"25 1","pages":"128"},"PeriodicalIF":3.3000,"publicationDate":"2025-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12067666/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unusual nodular goiter with recurrent laryngeal nerve palsy due to severe degeneration caused by intense chronic inflammation: a case report with histopathological evidence and review of the literature.\",\"authors\":\"Ryo Takagi, Kosei Mori, Sayumi Tsuyuguchi, Takashi Koike, Dinh Nam Nguyen, Kengo Kanai, Yoshihiro Watanabe, Mitsuhiro Okano, Yoshihiro Noguchi, Yuichiro Hayashi, Yorihisa Imanishi\",\"doi\":\"10.1186/s12902-025-01929-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Thyroid tumors presenting with recurrent laryngeal nerve (RLN) palsy are generally considered malignant; however, RLN palsy has been reported even in benign thyroid disease (BTD), mainly due to compression or stretching, although seemingly quite rare. Herein, we report an unusual case of nodular goiter that was extremely difficult to differentiate preoperatively from thyroid malignancy because of the concomitant ipsilateral RLN palsy caused by chronic inflammation.</p><p><strong>Case presentation: </strong>A 59-year-old Japanese female presented with hoarseness and pharyngeal discomfort. Endoscopic examination revealed fixation of the right vocal cord, presumably due to right RLN palsy. Ultrasonography and computed tomography showed an ill-defined thyroid mass lesion in the right lobe, strongly suggestive of malignancy, although repeated aspiration cytology revealed no suspicion of malignancy. Intraoperatively, because the right RLN was found to be entirely embedded within the hard mass lesion and completely unresponsive to nerve integrity monitoring, the nerve was unavoidably excised along with the right lobe. Histopathology led to the final diagnosis of nodular goiter, wherein the resected RLN was severely degenerated and disrupted due to intense chronic inflammation accompanied by perineural fibrosis.</p><p><strong>Conclusions: </strong>Our literature review suggests that RLN palsy associated with thyroid mass lesions should not be considered a definitive indicator of malignancy because it can also be observed in BTD, although it is significantly less frequent than in malignancy as corroborated by our meta-analysis. Even in BTD, if the primary cause of the coexisting RLN palsy is severe chronic inflammation, nerve preservation is potentially unfeasible.</p>\",\"PeriodicalId\":9152,\"journal\":{\"name\":\"BMC Endocrine Disorders\",\"volume\":\"25 1\",\"pages\":\"128\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-05-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12067666/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Endocrine Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12902-025-01929-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Endocrine Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12902-025-01929-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Unusual nodular goiter with recurrent laryngeal nerve palsy due to severe degeneration caused by intense chronic inflammation: a case report with histopathological evidence and review of the literature.
Background: Thyroid tumors presenting with recurrent laryngeal nerve (RLN) palsy are generally considered malignant; however, RLN palsy has been reported even in benign thyroid disease (BTD), mainly due to compression or stretching, although seemingly quite rare. Herein, we report an unusual case of nodular goiter that was extremely difficult to differentiate preoperatively from thyroid malignancy because of the concomitant ipsilateral RLN palsy caused by chronic inflammation.
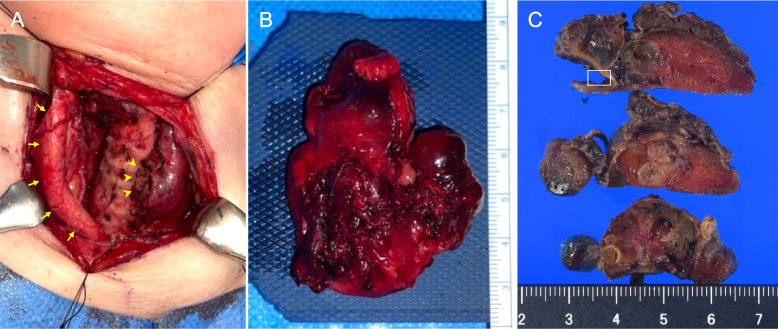
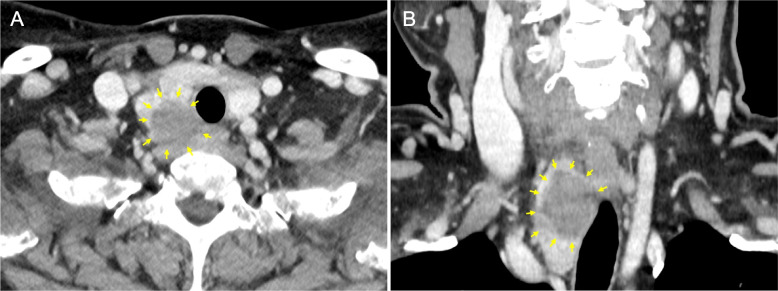
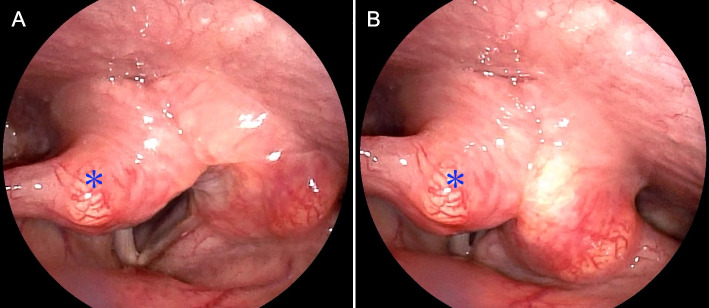
Case presentation: A 59-year-old Japanese female presented with hoarseness and pharyngeal discomfort. Endoscopic examination revealed fixation of the right vocal cord, presumably due to right RLN palsy. Ultrasonography and computed tomography showed an ill-defined thyroid mass lesion in the right lobe, strongly suggestive of malignancy, although repeated aspiration cytology revealed no suspicion of malignancy. Intraoperatively, because the right RLN was found to be entirely embedded within the hard mass lesion and completely unresponsive to nerve integrity monitoring, the nerve was unavoidably excised along with the right lobe. Histopathology led to the final diagnosis of nodular goiter, wherein the resected RLN was severely degenerated and disrupted due to intense chronic inflammation accompanied by perineural fibrosis.
Conclusions: Our literature review suggests that RLN palsy associated with thyroid mass lesions should not be considered a definitive indicator of malignancy because it can also be observed in BTD, although it is significantly less frequent than in malignancy as corroborated by our meta-analysis. Even in BTD, if the primary cause of the coexisting RLN palsy is severe chronic inflammation, nerve preservation is potentially unfeasible.
期刊介绍:
BMC Endocrine Disorders is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of endocrine disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


