Sara Villar, Emmanuel Curis, Marie-Hélène Schlageter, Nelly Bosselut, Amandine Charbonnier, Marie-Thérèse Rubio, Pascal Turlure, Hélène Labussière, Jacques-Olivier Bay, Jérome Cornillon, Laure Vincent, Corentin Orvain, Jean-Jacques Kiladjian, David Michonneau, Gérard Socié, Marie Robin
{"title":"移植前停用Ruxolitinib不会诱导骨髓纤维化的细胞因子释放。","authors":"Sara Villar, Emmanuel Curis, Marie-Hélène Schlageter, Nelly Bosselut, Amandine Charbonnier, Marie-Thérèse Rubio, Pascal Turlure, Hélène Labussière, Jacques-Olivier Bay, Jérome Cornillon, Laure Vincent, Corentin Orvain, Jean-Jacques Kiladjian, David Michonneau, Gérard Socié, Marie Robin","doi":"10.1007/s00262-025-04046-8","DOIUrl":null,"url":null,"abstract":"<p><p>Myelofibrosis (MF) is a myeloproliferative neoplasm characterized by marrow fibrosis, splenomegaly, constitutional symptoms and cytopenia with a proinflammatory and profibrotic cytokine phenotype involving the JAK-STAT pathway. Ruxolitinib is a JAK 1/2 inhibitor with proven efficacy on splenomegaly and constitutional symptoms, but it does not reverse fibrosis or the risk of leukemic transformation. While hematopoietic stem cell transplantation remains the only curative approach, it is still associated with a relatively high non-relapse mortality (NRM) rate, partly due to GVHD. The potential role of ruxolitinib or its withdrawal on NRM remains to be elucidated, and inflammatory cytokines might be implicated. In this report, we compared cytokine profiles in patients with myelofibrosis not treated with ruxolitinib (n = 18) or who received ruxolitinib and stopped it at conditioning regimen initiation (n = 53), at three different time points. At baseline, MF patients without ruxolitinib had increased inflammatory cytokine levels (CD25, REG3A, IL18 and ST2) as compared to MF patients on ruxolitinib. On day 0 and week 1 post-transplantation, levels of these cytokines were similar with and without ruxolitinib. On the other hand, cytokine levels at baseline did not predict grades 2-4 acute GVHD or hyperacute GVHD. These findings suggest that baseline cytokine profile in MF patients does not impact the risk of GVHD. Stopping ruxolitinib just before conditioning regimen may not influence GVHD risk more than in MF patients who have not received ruxolitinib. The potential benefit of a later ruxolitinib discontinuation on D0 or after transplantation ruxolitinib requires further investigation.</p>","PeriodicalId":9595,"journal":{"name":"Cancer Immunology, Immunotherapy","volume":"74 6","pages":"181"},"PeriodicalIF":5.1000,"publicationDate":"2025-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12022196/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ruxolitinib stopped before transplantation does not induce cytokine release in myelofibrosis.\",\"authors\":\"Sara Villar, Emmanuel Curis, Marie-Hélène Schlageter, Nelly Bosselut, Amandine Charbonnier, Marie-Thérèse Rubio, Pascal Turlure, Hélène Labussière, Jacques-Olivier Bay, Jérome Cornillon, Laure Vincent, Corentin Orvain, Jean-Jacques Kiladjian, David Michonneau, Gérard Socié, Marie Robin\",\"doi\":\"10.1007/s00262-025-04046-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Myelofibrosis (MF) is a myeloproliferative neoplasm characterized by marrow fibrosis, splenomegaly, constitutional symptoms and cytopenia with a proinflammatory and profibrotic cytokine phenotype involving the JAK-STAT pathway. Ruxolitinib is a JAK 1/2 inhibitor with proven efficacy on splenomegaly and constitutional symptoms, but it does not reverse fibrosis or the risk of leukemic transformation. While hematopoietic stem cell transplantation remains the only curative approach, it is still associated with a relatively high non-relapse mortality (NRM) rate, partly due to GVHD. The potential role of ruxolitinib or its withdrawal on NRM remains to be elucidated, and inflammatory cytokines might be implicated. In this report, we compared cytokine profiles in patients with myelofibrosis not treated with ruxolitinib (n = 18) or who received ruxolitinib and stopped it at conditioning regimen initiation (n = 53), at three different time points. At baseline, MF patients without ruxolitinib had increased inflammatory cytokine levels (CD25, REG3A, IL18 and ST2) as compared to MF patients on ruxolitinib. On day 0 and week 1 post-transplantation, levels of these cytokines were similar with and without ruxolitinib. On the other hand, cytokine levels at baseline did not predict grades 2-4 acute GVHD or hyperacute GVHD. These findings suggest that baseline cytokine profile in MF patients does not impact the risk of GVHD. Stopping ruxolitinib just before conditioning regimen may not influence GVHD risk more than in MF patients who have not received ruxolitinib. The potential benefit of a later ruxolitinib discontinuation on D0 or after transplantation ruxolitinib requires further investigation.</p>\",\"PeriodicalId\":9595,\"journal\":{\"name\":\"Cancer Immunology, Immunotherapy\",\"volume\":\"74 6\",\"pages\":\"181\"},\"PeriodicalIF\":5.1000,\"publicationDate\":\"2025-04-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12022196/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Immunology, Immunotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00262-025-04046-8\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Immunology, Immunotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00262-025-04046-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Ruxolitinib stopped before transplantation does not induce cytokine release in myelofibrosis.
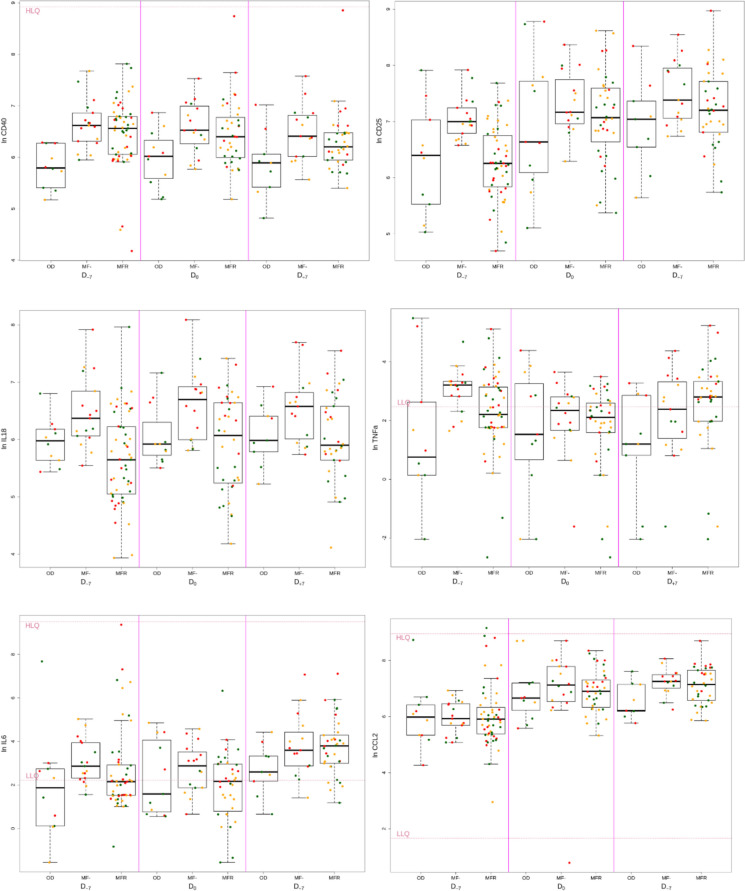
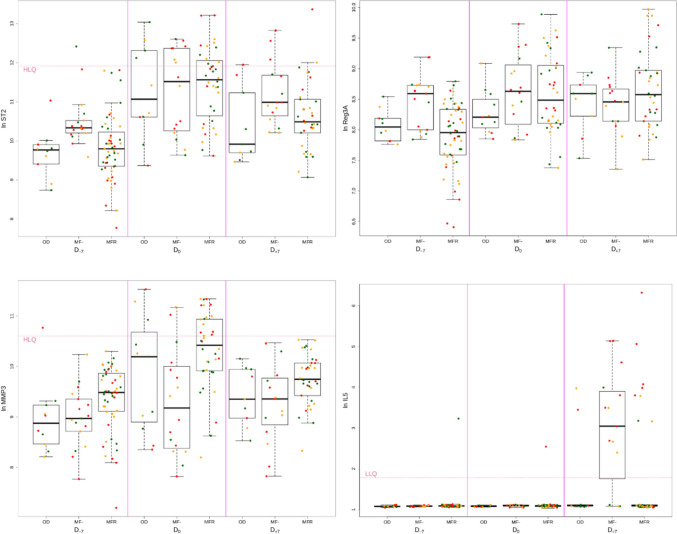
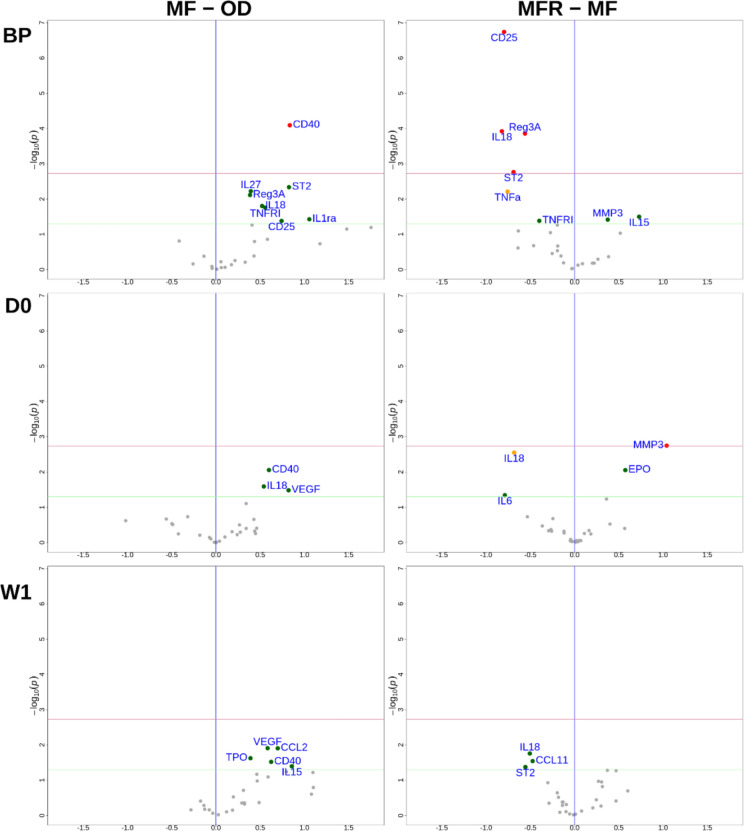
Myelofibrosis (MF) is a myeloproliferative neoplasm characterized by marrow fibrosis, splenomegaly, constitutional symptoms and cytopenia with a proinflammatory and profibrotic cytokine phenotype involving the JAK-STAT pathway. Ruxolitinib is a JAK 1/2 inhibitor with proven efficacy on splenomegaly and constitutional symptoms, but it does not reverse fibrosis or the risk of leukemic transformation. While hematopoietic stem cell transplantation remains the only curative approach, it is still associated with a relatively high non-relapse mortality (NRM) rate, partly due to GVHD. The potential role of ruxolitinib or its withdrawal on NRM remains to be elucidated, and inflammatory cytokines might be implicated. In this report, we compared cytokine profiles in patients with myelofibrosis not treated with ruxolitinib (n = 18) or who received ruxolitinib and stopped it at conditioning regimen initiation (n = 53), at three different time points. At baseline, MF patients without ruxolitinib had increased inflammatory cytokine levels (CD25, REG3A, IL18 and ST2) as compared to MF patients on ruxolitinib. On day 0 and week 1 post-transplantation, levels of these cytokines were similar with and without ruxolitinib. On the other hand, cytokine levels at baseline did not predict grades 2-4 acute GVHD or hyperacute GVHD. These findings suggest that baseline cytokine profile in MF patients does not impact the risk of GVHD. Stopping ruxolitinib just before conditioning regimen may not influence GVHD risk more than in MF patients who have not received ruxolitinib. The potential benefit of a later ruxolitinib discontinuation on D0 or after transplantation ruxolitinib requires further investigation.
期刊介绍:
Cancer Immunology, Immunotherapy has the basic aim of keeping readers informed of the latest research results in the fields of oncology and immunology. As knowledge expands, the scope of the journal has broadened to include more of the progress being made in the areas of biology concerned with biological response modifiers. This helps keep readers up to date on the latest advances in our understanding of tumor-host interactions.
The journal publishes short editorials including "position papers," general reviews, original articles, and short communications, providing a forum for the most current experimental and clinical advances in tumor immunology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


