{"title":"经内窥镜第三脑室造瘘治疗成人导水管狭窄后心室容积的纵向变化。","authors":"Florian Ebel, Caterina Mariani, Raphael Guzman, Jehuda Soleman","doi":"10.1186/s12987-025-00654-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Assessment of ventricular size following endoscopic third ventriculostomy (ETV) often relies on linear measurements and indexes such as the Evans index (EI) and frontal and occipital horn ratio (FOHR). Long-term data on ventricular volume following ETV is scarce, which leads to uncertainties regarding optimal follow-up duration and whether ventricular size correlates with clinical outcomes. This study aims to analyze the longitudinal changes of ventricular volume following ETV for aqueduct stenosis (AS) in adults.</p><p><strong>Methods: </strong>We retrospectively analyzed radiological images and clinical records of adult patients who underwent ETV for AS between the years 2010 and 2020. The primary endpoint was the change in lateral and third ventricular (LTV) volume at various follow-up periods in patients who did not require revision surgery (successful ETV group). Cluster analysis was performed to identify distinct volumetric patterns, and logistic regression was used to analyze the correlation between ventricular volume changes and clinical symptom improvement.</p><p><strong>Results: </strong>A total of 238 radiological images with 197 (82.8%) MRI and 41 (17.2%) CT scans from 46 patients were analyzed. Thirty-nine (84.8%) patients did not require revision surgery (successful ETV group). In the successful ETV group, LTV volume decreased by 19.6% within 3 months, 31% after 3-6 months, and 47.5% after 6-12 months. Two main clusters were identified: one with a mean LTV volume decrease of 56% and the other of 18.9% after 1 year. The presence of a pineal or tectal lesion (OR 3.94, p = 0.074) tended to be predictive of the former cluster, and the presence of a membrane in the aqueduct (OR 5.1, p = 0.036) was predictive of the latter. Volumetric changes were significantly greater than those measured by EI and FOHR postoperatively (p < 0.001) and at the last follow-up (p = 0.002). There was no association between LTV volume reduction and clinical improvement during the follow-up period (OR 1.03, [95% CI 0.99-1.06]; p = 0.195).</p><p><strong>Conclusion: </strong>Volumetric analysis provides a more accurate representation of ventricular size changes following ETV for AS. It demonstrates a continuous reduction in LTV volume during the first year after surgery, whereafter LTV volume appears to stabilize with a cumulative reduction of 38.7%, suggesting that lifelong imaging may be unnecessary in these patients. However, it does not predict the clinical outcome.</p>","PeriodicalId":12321,"journal":{"name":"Fluids and Barriers of the CNS","volume":"22 1","pages":"42"},"PeriodicalIF":6.2000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12023378/pdf/","citationCount":"0","resultStr":"{\"title\":\"Longitudinal changes in ventricular volume after treating aqueduct stenosis through endoscopic third ventriculostomy in adults.\",\"authors\":\"Florian Ebel, Caterina Mariani, Raphael Guzman, Jehuda Soleman\",\"doi\":\"10.1186/s12987-025-00654-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Assessment of ventricular size following endoscopic third ventriculostomy (ETV) often relies on linear measurements and indexes such as the Evans index (EI) and frontal and occipital horn ratio (FOHR). Long-term data on ventricular volume following ETV is scarce, which leads to uncertainties regarding optimal follow-up duration and whether ventricular size correlates with clinical outcomes. This study aims to analyze the longitudinal changes of ventricular volume following ETV for aqueduct stenosis (AS) in adults.</p><p><strong>Methods: </strong>We retrospectively analyzed radiological images and clinical records of adult patients who underwent ETV for AS between the years 2010 and 2020. The primary endpoint was the change in lateral and third ventricular (LTV) volume at various follow-up periods in patients who did not require revision surgery (successful ETV group). Cluster analysis was performed to identify distinct volumetric patterns, and logistic regression was used to analyze the correlation between ventricular volume changes and clinical symptom improvement.</p><p><strong>Results: </strong>A total of 238 radiological images with 197 (82.8%) MRI and 41 (17.2%) CT scans from 46 patients were analyzed. Thirty-nine (84.8%) patients did not require revision surgery (successful ETV group). In the successful ETV group, LTV volume decreased by 19.6% within 3 months, 31% after 3-6 months, and 47.5% after 6-12 months. Two main clusters were identified: one with a mean LTV volume decrease of 56% and the other of 18.9% after 1 year. The presence of a pineal or tectal lesion (OR 3.94, p = 0.074) tended to be predictive of the former cluster, and the presence of a membrane in the aqueduct (OR 5.1, p = 0.036) was predictive of the latter. Volumetric changes were significantly greater than those measured by EI and FOHR postoperatively (p < 0.001) and at the last follow-up (p = 0.002). There was no association between LTV volume reduction and clinical improvement during the follow-up period (OR 1.03, [95% CI 0.99-1.06]; p = 0.195).</p><p><strong>Conclusion: </strong>Volumetric analysis provides a more accurate representation of ventricular size changes following ETV for AS. It demonstrates a continuous reduction in LTV volume during the first year after surgery, whereafter LTV volume appears to stabilize with a cumulative reduction of 38.7%, suggesting that lifelong imaging may be unnecessary in these patients. However, it does not predict the clinical outcome.</p>\",\"PeriodicalId\":12321,\"journal\":{\"name\":\"Fluids and Barriers of the CNS\",\"volume\":\"22 1\",\"pages\":\"42\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12023378/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Fluids and Barriers of the CNS\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12987-025-00654-9\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"NEUROSCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Fluids and Barriers of the CNS","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12987-025-00654-9","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
摘要
背景:内镜下第三脑室造口术(ETV)后心室大小的评估通常依赖于线性测量和指标,如埃文斯指数(EI)和额枕角比(FOHR)。ETV术后心室容量的长期数据很少,这导致了最佳随访时间和心室大小是否与临床结果相关的不确定性。本研究旨在分析成人导水管狭窄(AS)行ETV后心室容积的纵向变化。方法:我们回顾性分析2010年至2020年间接受AS ETV治疗的成年患者的影像学和临床记录。主要终点是不需要翻修手术的患者(成功的ETV组)在不同随访期间侧室和第三心室(LTV)体积的变化。采用聚类分析确定不同的容积模式,并采用logistic回归分析心室容积变化与临床症状改善之间的相关性。结果:分析46例患者238张影像学图像,其中MRI扫描197张(82.8%),CT扫描41张(17.2%)。39例(84.8%)患者不需要翻修手术(ETV成功组)。在成功的ETV组中,LTV量在3个月内下降了19.6%,3-6个月下降了31%,6-12个月下降了47.5%。确定了两个主要集群:一年后平均LTV体积下降56%,另一个下降18.9%。松果体或顶部病变(or 3.94, p = 0.074)倾向于预测前一组,而导水管膜的存在(or 5.1, p = 0.036)倾向于预测后一组。体积变化明显大于术后EI和FOHR测量的结果(p结论:体积分析可以更准确地反映AS患者ETV后心室大小的变化。研究显示,术后第一年LTV体积持续减少,此后LTV体积趋于稳定,累计减少38.7%,表明这些患者可能不需要终身影像学检查。然而,它不能预测临床结果。
Longitudinal changes in ventricular volume after treating aqueduct stenosis through endoscopic third ventriculostomy in adults.
Background: Assessment of ventricular size following endoscopic third ventriculostomy (ETV) often relies on linear measurements and indexes such as the Evans index (EI) and frontal and occipital horn ratio (FOHR). Long-term data on ventricular volume following ETV is scarce, which leads to uncertainties regarding optimal follow-up duration and whether ventricular size correlates with clinical outcomes. This study aims to analyze the longitudinal changes of ventricular volume following ETV for aqueduct stenosis (AS) in adults.
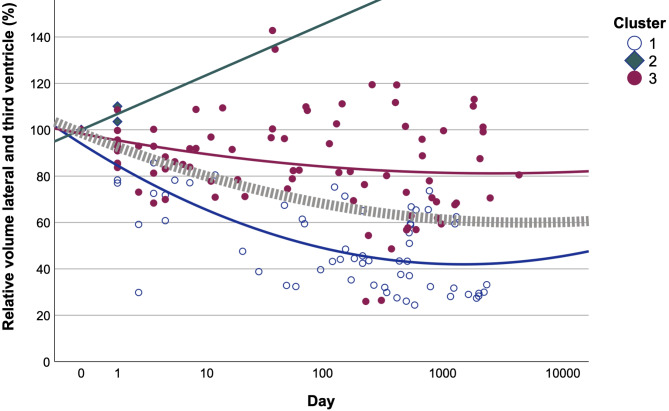
Methods: We retrospectively analyzed radiological images and clinical records of adult patients who underwent ETV for AS between the years 2010 and 2020. The primary endpoint was the change in lateral and third ventricular (LTV) volume at various follow-up periods in patients who did not require revision surgery (successful ETV group). Cluster analysis was performed to identify distinct volumetric patterns, and logistic regression was used to analyze the correlation between ventricular volume changes and clinical symptom improvement.
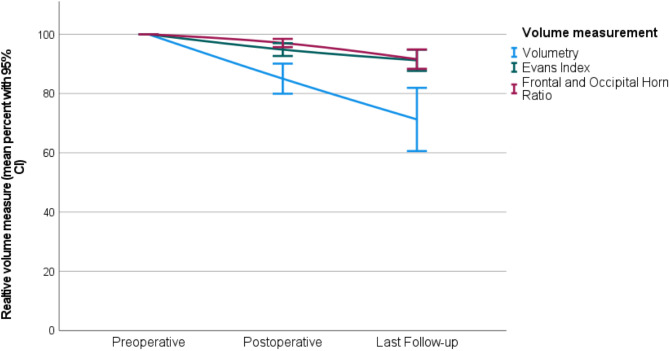
Results: A total of 238 radiological images with 197 (82.8%) MRI and 41 (17.2%) CT scans from 46 patients were analyzed. Thirty-nine (84.8%) patients did not require revision surgery (successful ETV group). In the successful ETV group, LTV volume decreased by 19.6% within 3 months, 31% after 3-6 months, and 47.5% after 6-12 months. Two main clusters were identified: one with a mean LTV volume decrease of 56% and the other of 18.9% after 1 year. The presence of a pineal or tectal lesion (OR 3.94, p = 0.074) tended to be predictive of the former cluster, and the presence of a membrane in the aqueduct (OR 5.1, p = 0.036) was predictive of the latter. Volumetric changes were significantly greater than those measured by EI and FOHR postoperatively (p < 0.001) and at the last follow-up (p = 0.002). There was no association between LTV volume reduction and clinical improvement during the follow-up period (OR 1.03, [95% CI 0.99-1.06]; p = 0.195).
Conclusion: Volumetric analysis provides a more accurate representation of ventricular size changes following ETV for AS. It demonstrates a continuous reduction in LTV volume during the first year after surgery, whereafter LTV volume appears to stabilize with a cumulative reduction of 38.7%, suggesting that lifelong imaging may be unnecessary in these patients. However, it does not predict the clinical outcome.
期刊介绍:
"Fluids and Barriers of the CNS" is a scholarly open access journal that specializes in the intricate world of the central nervous system's fluids and barriers, which are pivotal for the health and well-being of the human body. This journal is a peer-reviewed platform that welcomes research manuscripts exploring the full spectrum of CNS fluids and barriers, with a particular focus on their roles in both health and disease.
At the heart of this journal's interest is the cerebrospinal fluid (CSF), a vital fluid that circulates within the brain and spinal cord, playing a multifaceted role in the normal functioning of the brain and in various neurological conditions. The journal delves into the composition, circulation, and absorption of CSF, as well as its relationship with the parenchymal interstitial fluid and the neurovascular unit at the blood-brain barrier (BBB).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


