Ramona Paula Fernandes Reckziegel, Lenara Golbert, Erika Laurini de Souza Meyer
{"title":"术前促甲状腺激素水平在预测甲状腺切除术后甲状腺激素替代中的作用。","authors":"Ramona Paula Fernandes Reckziegel, Lenara Golbert, Erika Laurini de Souza Meyer","doi":"10.1055/s-0045-1801852","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b> Hemithyroidectomy is performed for the treatment of symptomatic unilateral benign nodules, cytologically indeterminate nodules, and some cases of well-differentiated thyroid cancer. <b>Objective</b> To evaluate the frequency of postlobectomy thyroid hormone replacement (THR), and to analyze the clinical-pathological factors predicting L-thyroxine (T4) use in patients undergoing hemithyroidectomy. <b>Methods</b> We conducted an observational, retrospective study in which clinical, biochemical, and anatomopathological parameters were analyzed and correlated with the need for THR after thyroid lobectomy. <b>Results</b> The frequency of postoperative THR was 63%. The preoperative thyroid-stimulating hormone (TSH) level was an important predictor of postoperative THR. When stratifying preoperative TSH levels, the frequencies of T4 replacement in each TSH quartile varied, being more frequent with increasing presurgical TSH levels ( <i>p</i> = 0.029). The preoperative cutoff that maximized sensitivity and specificity for the development of hypothyroidism was 1.21 μIU/mL. <b>Conclusion</b> Our results demonstrated a significant frequency of postlobectomy THR. Higher preoperative TSH is a strong risk factor for postsurgical hypothyroidism, and even lower preoperative levels within the normal references do not exclude the risk of thyroid hormone use after thyroid lobectomy.</p>","PeriodicalId":13731,"journal":{"name":"International Archives of Otorhinolaryngology","volume":"29 2","pages":"1-6"},"PeriodicalIF":1.1000,"publicationDate":"2025-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020584/pdf/","citationCount":"0","resultStr":"{\"title\":\"Role of Preoperative Thyroid-Stimulating Hormone Levels in the Prediction of Thyroid Hormone Replacement after Hemithyroidectomy.\",\"authors\":\"Ramona Paula Fernandes Reckziegel, Lenara Golbert, Erika Laurini de Souza Meyer\",\"doi\":\"10.1055/s-0045-1801852\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b> Hemithyroidectomy is performed for the treatment of symptomatic unilateral benign nodules, cytologically indeterminate nodules, and some cases of well-differentiated thyroid cancer. <b>Objective</b> To evaluate the frequency of postlobectomy thyroid hormone replacement (THR), and to analyze the clinical-pathological factors predicting L-thyroxine (T4) use in patients undergoing hemithyroidectomy. <b>Methods</b> We conducted an observational, retrospective study in which clinical, biochemical, and anatomopathological parameters were analyzed and correlated with the need for THR after thyroid lobectomy. <b>Results</b> The frequency of postoperative THR was 63%. The preoperative thyroid-stimulating hormone (TSH) level was an important predictor of postoperative THR. When stratifying preoperative TSH levels, the frequencies of T4 replacement in each TSH quartile varied, being more frequent with increasing presurgical TSH levels ( <i>p</i> = 0.029). The preoperative cutoff that maximized sensitivity and specificity for the development of hypothyroidism was 1.21 μIU/mL. <b>Conclusion</b> Our results demonstrated a significant frequency of postlobectomy THR. Higher preoperative TSH is a strong risk factor for postsurgical hypothyroidism, and even lower preoperative levels within the normal references do not exclude the risk of thyroid hormone use after thyroid lobectomy.</p>\",\"PeriodicalId\":13731,\"journal\":{\"name\":\"International Archives of Otorhinolaryngology\",\"volume\":\"29 2\",\"pages\":\"1-6\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2025-04-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020584/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Archives of Otorhinolaryngology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0045-1801852\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Archives of Otorhinolaryngology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1801852","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
Role of Preoperative Thyroid-Stimulating Hormone Levels in the Prediction of Thyroid Hormone Replacement after Hemithyroidectomy.
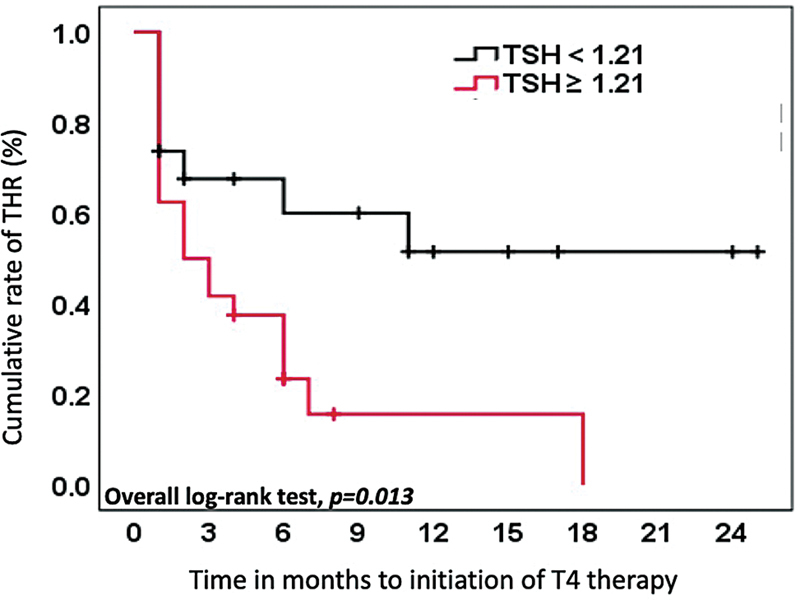
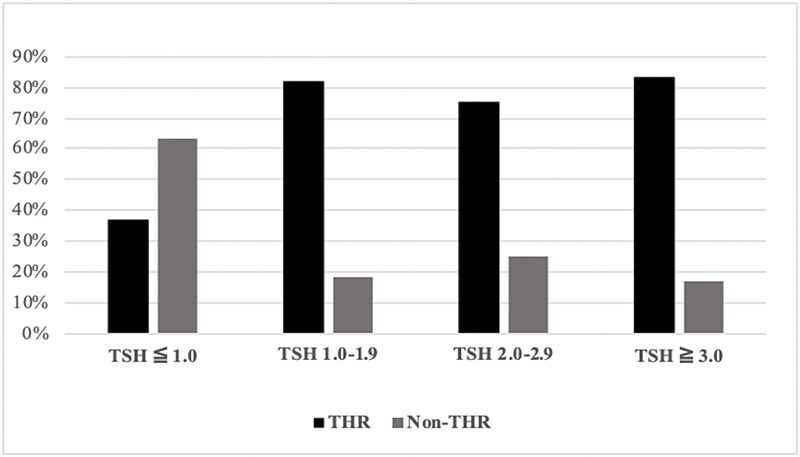
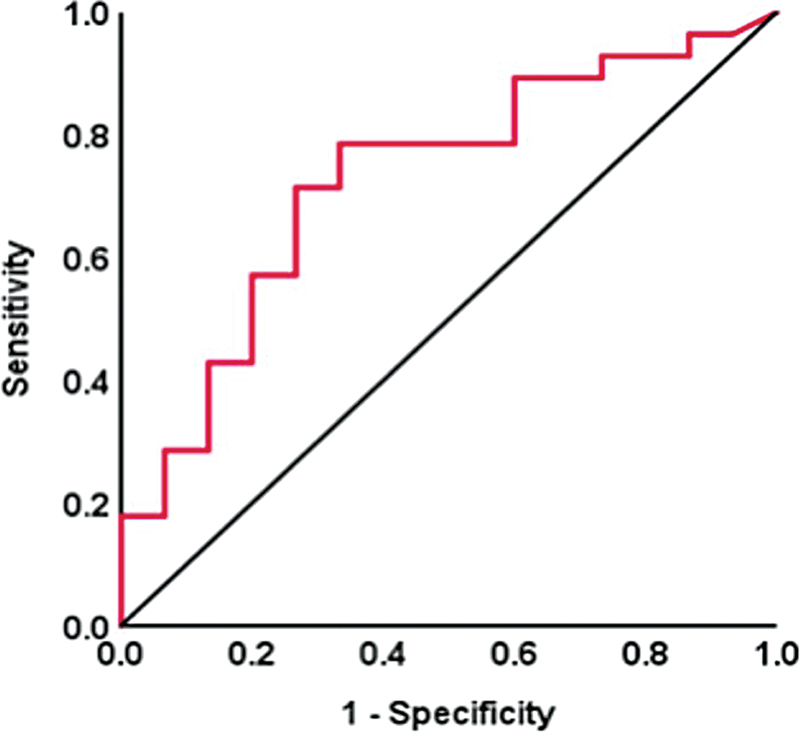
Introduction Hemithyroidectomy is performed for the treatment of symptomatic unilateral benign nodules, cytologically indeterminate nodules, and some cases of well-differentiated thyroid cancer. Objective To evaluate the frequency of postlobectomy thyroid hormone replacement (THR), and to analyze the clinical-pathological factors predicting L-thyroxine (T4) use in patients undergoing hemithyroidectomy. Methods We conducted an observational, retrospective study in which clinical, biochemical, and anatomopathological parameters were analyzed and correlated with the need for THR after thyroid lobectomy. Results The frequency of postoperative THR was 63%. The preoperative thyroid-stimulating hormone (TSH) level was an important predictor of postoperative THR. When stratifying preoperative TSH levels, the frequencies of T4 replacement in each TSH quartile varied, being more frequent with increasing presurgical TSH levels ( p = 0.029). The preoperative cutoff that maximized sensitivity and specificity for the development of hypothyroidism was 1.21 μIU/mL. Conclusion Our results demonstrated a significant frequency of postlobectomy THR. Higher preoperative TSH is a strong risk factor for postsurgical hypothyroidism, and even lower preoperative levels within the normal references do not exclude the risk of thyroid hormone use after thyroid lobectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


