{"title":"HIV/AIDS患者播散性组织胞浆菌病引起的发热性全血细胞减少和噬血症:2例及抗真菌和类固醇联合治疗的综述。","authors":"Chinelo Animalu, Nupur Singh, Kenneth Cory Guice, Kase Maner","doi":"10.1155/crdi/2623694","DOIUrl":null,"url":null,"abstract":"<p><p>Hemophagocytosis is a clinical condition characterized by the engulfment of bone marrow cellular elements, including erythrocytes, leukocytes, platelets, and their precursors, by activated macrophages. It has been associated with several infectious organisms, including the Epstein-Barr virus (EBV) and histoplasmosis. Human immunodeficiency virus (HIV) has been known to trigger hemophagocytosis in the presence or absence of other infections. Disseminated histoplasmosis is a common opportunistic infection in advanced patients with acquired immunodeficiency syndrome (AIDS) in endemic areas; however, the best treatment for histoplasmosis associated with hemophagocytosis is uncertain. This article presents two cases of patients with AIDS secondary to uncontrolled HIV who were admitted with fever, malaise, low CD4 + counts, and a history of noncompliance with antiretroviral therapy (ART). Both patients had pancytopenia, markedly elevated serum ferritin, and elevated liver transaminases. The diagnosis of histoplasmosis was confirmed by positive fungal blood cultures, buffy coat smears showing intracellular fungal organisms, and positive urine <i>Histoplasma</i> antigen. Bone marrow biopsies revealed <i>Histoplasma capsulatum</i> (<i>H. capsulatum</i>) in Grocott methenamine silver (GMS) stains and fungal cultures, histiocytes with intracellular red blood cells, and precursors of granulocytes, consistent with hemophagocytosis. Both patients received amphotericin B but remained febrile and pancytopenic, eventually requiring corticosteroid therapy. We present our experience with these patients and discuss the management of hemophagocytosis in patients with AIDS with disseminated histoplasmosis. We also completed a literature review and created a list of all known cases of disseminated histoplasmosis complicated by HIV/AIDS and hemophagocytosis and listed previous treatments.</p>","PeriodicalId":9608,"journal":{"name":"Case Reports in Infectious Diseases","volume":"2025 ","pages":"2623694"},"PeriodicalIF":0.8000,"publicationDate":"2025-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12021483/pdf/","citationCount":"0","resultStr":"{\"title\":\"Febrile Pancytopenia and Hemophagocytosis From Disseminated Histoplasmosis in HIV/AIDS Patients: Two Cases and a Review of Combined Antifungal and Steroid Therapy.\",\"authors\":\"Chinelo Animalu, Nupur Singh, Kenneth Cory Guice, Kase Maner\",\"doi\":\"10.1155/crdi/2623694\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Hemophagocytosis is a clinical condition characterized by the engulfment of bone marrow cellular elements, including erythrocytes, leukocytes, platelets, and their precursors, by activated macrophages. It has been associated with several infectious organisms, including the Epstein-Barr virus (EBV) and histoplasmosis. Human immunodeficiency virus (HIV) has been known to trigger hemophagocytosis in the presence or absence of other infections. Disseminated histoplasmosis is a common opportunistic infection in advanced patients with acquired immunodeficiency syndrome (AIDS) in endemic areas; however, the best treatment for histoplasmosis associated with hemophagocytosis is uncertain. This article presents two cases of patients with AIDS secondary to uncontrolled HIV who were admitted with fever, malaise, low CD4 + counts, and a history of noncompliance with antiretroviral therapy (ART). Both patients had pancytopenia, markedly elevated serum ferritin, and elevated liver transaminases. The diagnosis of histoplasmosis was confirmed by positive fungal blood cultures, buffy coat smears showing intracellular fungal organisms, and positive urine <i>Histoplasma</i> antigen. Bone marrow biopsies revealed <i>Histoplasma capsulatum</i> (<i>H. capsulatum</i>) in Grocott methenamine silver (GMS) stains and fungal cultures, histiocytes with intracellular red blood cells, and precursors of granulocytes, consistent with hemophagocytosis. Both patients received amphotericin B but remained febrile and pancytopenic, eventually requiring corticosteroid therapy. We present our experience with these patients and discuss the management of hemophagocytosis in patients with AIDS with disseminated histoplasmosis. We also completed a literature review and created a list of all known cases of disseminated histoplasmosis complicated by HIV/AIDS and hemophagocytosis and listed previous treatments.</p>\",\"PeriodicalId\":9608,\"journal\":{\"name\":\"Case Reports in Infectious Diseases\",\"volume\":\"2025 \",\"pages\":\"2623694\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2025-04-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12021483/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Infectious Diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crdi/2623694\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Infectious Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crdi/2623694","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Febrile Pancytopenia and Hemophagocytosis From Disseminated Histoplasmosis in HIV/AIDS Patients: Two Cases and a Review of Combined Antifungal and Steroid Therapy.
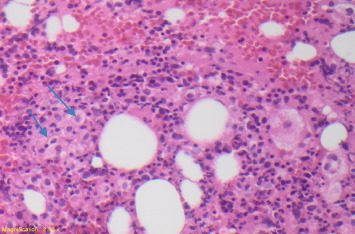
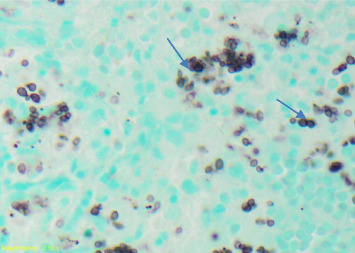
Hemophagocytosis is a clinical condition characterized by the engulfment of bone marrow cellular elements, including erythrocytes, leukocytes, platelets, and their precursors, by activated macrophages. It has been associated with several infectious organisms, including the Epstein-Barr virus (EBV) and histoplasmosis. Human immunodeficiency virus (HIV) has been known to trigger hemophagocytosis in the presence or absence of other infections. Disseminated histoplasmosis is a common opportunistic infection in advanced patients with acquired immunodeficiency syndrome (AIDS) in endemic areas; however, the best treatment for histoplasmosis associated with hemophagocytosis is uncertain. This article presents two cases of patients with AIDS secondary to uncontrolled HIV who were admitted with fever, malaise, low CD4 + counts, and a history of noncompliance with antiretroviral therapy (ART). Both patients had pancytopenia, markedly elevated serum ferritin, and elevated liver transaminases. The diagnosis of histoplasmosis was confirmed by positive fungal blood cultures, buffy coat smears showing intracellular fungal organisms, and positive urine Histoplasma antigen. Bone marrow biopsies revealed Histoplasma capsulatum (H. capsulatum) in Grocott methenamine silver (GMS) stains and fungal cultures, histiocytes with intracellular red blood cells, and precursors of granulocytes, consistent with hemophagocytosis. Both patients received amphotericin B but remained febrile and pancytopenic, eventually requiring corticosteroid therapy. We present our experience with these patients and discuss the management of hemophagocytosis in patients with AIDS with disseminated histoplasmosis. We also completed a literature review and created a list of all known cases of disseminated histoplasmosis complicated by HIV/AIDS and hemophagocytosis and listed previous treatments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


