Heitor J S Medeiros, Amanda Cyntia Lima Fonseca Rodrigue, Ariel Mueller, Elizabeth Korn, A Sassan Sabouri
{"title":"胸骨旁肋间平面阻滞用于成人心脏手术胸骨中线切开术的镇痛效果:随机对照试验的系统回顾和荟萃分析。","authors":"Heitor J S Medeiros, Amanda Cyntia Lima Fonseca Rodrigue, Ariel Mueller, Elizabeth Korn, A Sassan Sabouri","doi":"10.14440/jbm.2024.0070","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Regional anesthesia is widely supported as a part of multimodal analgesia for post-operative pain management following cardiac surgery. A common technique for managing post-sternotomy pain is the parasternal intercostal plane (PIP) block, which involves injecting anesthetics into the fascial planes near the sternum to block the anterior cutaneous branches of the T2 - T6 nerves.</p><p><strong>Objective: </strong>This study aimed to assess the effects of PIP blocks on post-sternotomy pain, narcotic usage, intensive care unit (ICU) stay, and extubation time following adult cardiac surgeries.</p><p><strong>Methodology: </strong>We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) investigating PIP blocks in adult cardiac surgery with midline sternotomy. Studies were retrieved from PubMed, Cochrane Library, and Embase through February 22, 2023. The risk of bias (ROB) in RCTs was assessed using the Cochrane ROB tool, version 2. Twelve RCTs involving 819 adult patients were included. Primary outcomes were pain scores at 12 and 24 h post-surgery and narcotic usage in morphine milligram equivalents (MME). Secondary outcomes included extubation time and ICU stay.</p><p><strong>Results: </strong>The PIP block group had significantly lower pain scores at 12 (mean difference [MD]: -1.21 points, 95% confidence interval [CI]: -2.17, -0.25, <i>p</i> = 0.013) and 24 hours (MD: -0.69 points, 95% CI: -1.35, -0.02, <i>p</i> = 0.042), and reduced MME use (MD: -30.34 MME, 95% CI: -45.80, -14.89, <i>p</i> < 0.001). PIP blocks did not significantly reduce extubation time (MD: -0.77 h, 95% CI: -1.64, 0.09, <i>p</i> = 0.080) but were associated with shorter ICU stay (MD: -0.54 days, 95% CI: -0.94, -0.13, <i>p</i> = 0.009).</p><p><strong>Conclusion: </strong>PIP blocks provided effective analgesia and reduced ICU stay in cardiac surgery patients requiring sternotomy, but due to study heterogeneity, results should be interpreted with caution. Future research is warranted to explore its short- and long-term outcomes.</p>","PeriodicalId":73618,"journal":{"name":"Journal of biological methods","volume":"12 1","pages":"e99010033"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11973045/pdf/","citationCount":"0","resultStr":"{\"title\":\"Analgesic efficacy of parasternal intercostal plane block for midline sternotomy in adult cardiac surgery: A systematic review and meta-analysis of randomized controlled trials.\",\"authors\":\"Heitor J S Medeiros, Amanda Cyntia Lima Fonseca Rodrigue, Ariel Mueller, Elizabeth Korn, A Sassan Sabouri\",\"doi\":\"10.14440/jbm.2024.0070\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Regional anesthesia is widely supported as a part of multimodal analgesia for post-operative pain management following cardiac surgery. A common technique for managing post-sternotomy pain is the parasternal intercostal plane (PIP) block, which involves injecting anesthetics into the fascial planes near the sternum to block the anterior cutaneous branches of the T2 - T6 nerves.</p><p><strong>Objective: </strong>This study aimed to assess the effects of PIP blocks on post-sternotomy pain, narcotic usage, intensive care unit (ICU) stay, and extubation time following adult cardiac surgeries.</p><p><strong>Methodology: </strong>We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) investigating PIP blocks in adult cardiac surgery with midline sternotomy. Studies were retrieved from PubMed, Cochrane Library, and Embase through February 22, 2023. The risk of bias (ROB) in RCTs was assessed using the Cochrane ROB tool, version 2. Twelve RCTs involving 819 adult patients were included. Primary outcomes were pain scores at 12 and 24 h post-surgery and narcotic usage in morphine milligram equivalents (MME). Secondary outcomes included extubation time and ICU stay.</p><p><strong>Results: </strong>The PIP block group had significantly lower pain scores at 12 (mean difference [MD]: -1.21 points, 95% confidence interval [CI]: -2.17, -0.25, <i>p</i> = 0.013) and 24 hours (MD: -0.69 points, 95% CI: -1.35, -0.02, <i>p</i> = 0.042), and reduced MME use (MD: -30.34 MME, 95% CI: -45.80, -14.89, <i>p</i> < 0.001). PIP blocks did not significantly reduce extubation time (MD: -0.77 h, 95% CI: -1.64, 0.09, <i>p</i> = 0.080) but were associated with shorter ICU stay (MD: -0.54 days, 95% CI: -0.94, -0.13, <i>p</i> = 0.009).</p><p><strong>Conclusion: </strong>PIP blocks provided effective analgesia and reduced ICU stay in cardiac surgery patients requiring sternotomy, but due to study heterogeneity, results should be interpreted with caution. Future research is warranted to explore its short- and long-term outcomes.</p>\",\"PeriodicalId\":73618,\"journal\":{\"name\":\"Journal of biological methods\",\"volume\":\"12 1\",\"pages\":\"e99010033\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11973045/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of biological methods\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14440/jbm.2024.0070\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of biological methods","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14440/jbm.2024.0070","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Analgesic efficacy of parasternal intercostal plane block for midline sternotomy in adult cardiac surgery: A systematic review and meta-analysis of randomized controlled trials.
Background: Regional anesthesia is widely supported as a part of multimodal analgesia for post-operative pain management following cardiac surgery. A common technique for managing post-sternotomy pain is the parasternal intercostal plane (PIP) block, which involves injecting anesthetics into the fascial planes near the sternum to block the anterior cutaneous branches of the T2 - T6 nerves.
Objective: This study aimed to assess the effects of PIP blocks on post-sternotomy pain, narcotic usage, intensive care unit (ICU) stay, and extubation time following adult cardiac surgeries.
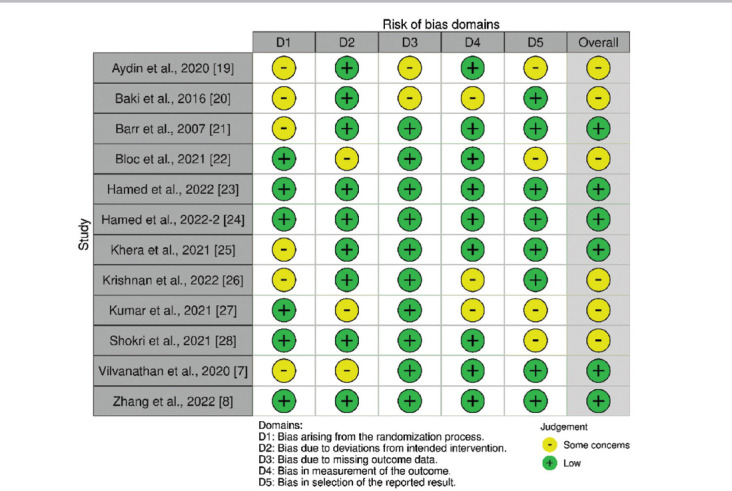
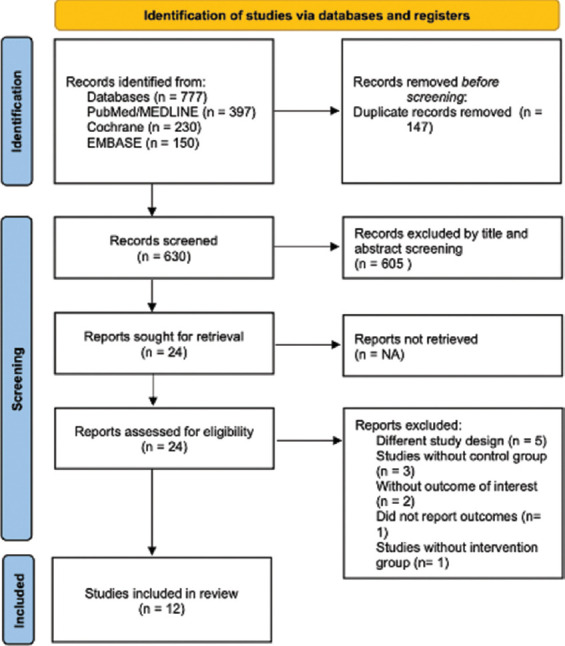
Methodology: We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) investigating PIP blocks in adult cardiac surgery with midline sternotomy. Studies were retrieved from PubMed, Cochrane Library, and Embase through February 22, 2023. The risk of bias (ROB) in RCTs was assessed using the Cochrane ROB tool, version 2. Twelve RCTs involving 819 adult patients were included. Primary outcomes were pain scores at 12 and 24 h post-surgery and narcotic usage in morphine milligram equivalents (MME). Secondary outcomes included extubation time and ICU stay.
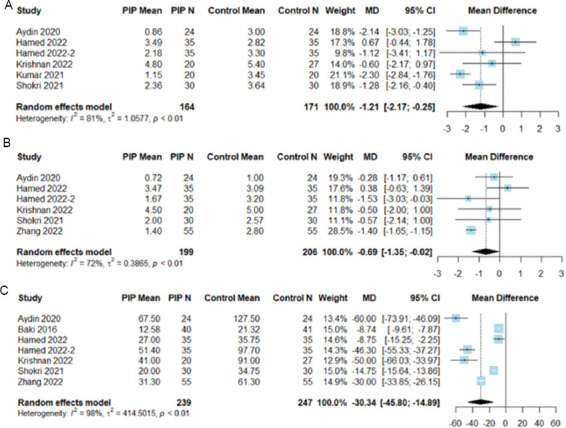
Results: The PIP block group had significantly lower pain scores at 12 (mean difference [MD]: -1.21 points, 95% confidence interval [CI]: -2.17, -0.25, p = 0.013) and 24 hours (MD: -0.69 points, 95% CI: -1.35, -0.02, p = 0.042), and reduced MME use (MD: -30.34 MME, 95% CI: -45.80, -14.89, p < 0.001). PIP blocks did not significantly reduce extubation time (MD: -0.77 h, 95% CI: -1.64, 0.09, p = 0.080) but were associated with shorter ICU stay (MD: -0.54 days, 95% CI: -0.94, -0.13, p = 0.009).
Conclusion: PIP blocks provided effective analgesia and reduced ICU stay in cardiac surgery patients requiring sternotomy, but due to study heterogeneity, results should be interpreted with caution. Future research is warranted to explore its short- and long-term outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


