Cassandra Mackey, Simi Jandu, James Fidrocki, Tyler Raduzycki, Jennifer Carey
{"title":"探索医学模拟学习的最佳小组规模:系统回顾。","authors":"Cassandra Mackey, Simi Jandu, James Fidrocki, Tyler Raduzycki, Jennifer Carey","doi":"10.1177/23821205251327287","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Simulation is an effective teaching method that improves learner competence and confidence. Optimizing group size balances efficiency without sacrificing efficacy. While simulation technology is widely used in medical education, no standard for learner group size exists. This study investigates the optimal group size for simulation, aiming to identify best practices that maximize efficiency and efficacy in learning environments.</p><p><strong>Methods: </strong>This systematic review adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. A team of emergency medicine educators screened citations and reviewed relevant full-text articles. Inclusion criteria focused on group sizes with the best outcomes. Quality assessment employed the Medical Education Research Study Quality Instrument approach to evaluate evidence.</p><p><strong>Results: </strong>Thirty-four articles were identified; 17 were deemed relevant for full-text review. The studies varied in methods, including prospective and retrospective reviews, mixed methods, and randomized controlled trials. Smaller groups improved outcomes, with an ideal size dependent on learning objectives. Five studies suggested groups of up to 4 learners were optimal, with mixed results on the exact number. One study identified 6 as the ideal group size. Debriefing was effective in larger groups, while procedural skills were best taught in groups of 2 to 4 learners.</p><p><strong>Conclusion: </strong>This review suggests smaller group sizes are more effective for efficiency, knowledge, and confidence. For procedural skills, groups of 2 to 4 are most effective, and effectiveness declines with more than 6 participants. Smaller groups allow for more hands-on learning and cognitive engagement. While clinical skills can be taught in larger groups, learners favor smaller groups for debriefing and complex scenarios. Effective curriculum planning should account for available resources, the type of simulation, and the material being taught, with group sizes adjusted to optimize learning outcomes.</p>","PeriodicalId":45121,"journal":{"name":"Journal of Medical Education and Curricular Development","volume":"12 ","pages":"23821205251327287"},"PeriodicalIF":1.6000,"publicationDate":"2025-04-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11970070/pdf/","citationCount":"0","resultStr":"{\"title\":\"Exploring Optimal Group Sizes for Learning in Medical Simulation: A Systematic Review.\",\"authors\":\"Cassandra Mackey, Simi Jandu, James Fidrocki, Tyler Raduzycki, Jennifer Carey\",\"doi\":\"10.1177/23821205251327287\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Simulation is an effective teaching method that improves learner competence and confidence. Optimizing group size balances efficiency without sacrificing efficacy. While simulation technology is widely used in medical education, no standard for learner group size exists. This study investigates the optimal group size for simulation, aiming to identify best practices that maximize efficiency and efficacy in learning environments.</p><p><strong>Methods: </strong>This systematic review adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. A team of emergency medicine educators screened citations and reviewed relevant full-text articles. Inclusion criteria focused on group sizes with the best outcomes. Quality assessment employed the Medical Education Research Study Quality Instrument approach to evaluate evidence.</p><p><strong>Results: </strong>Thirty-four articles were identified; 17 were deemed relevant for full-text review. The studies varied in methods, including prospective and retrospective reviews, mixed methods, and randomized controlled trials. Smaller groups improved outcomes, with an ideal size dependent on learning objectives. Five studies suggested groups of up to 4 learners were optimal, with mixed results on the exact number. One study identified 6 as the ideal group size. Debriefing was effective in larger groups, while procedural skills were best taught in groups of 2 to 4 learners.</p><p><strong>Conclusion: </strong>This review suggests smaller group sizes are more effective for efficiency, knowledge, and confidence. For procedural skills, groups of 2 to 4 are most effective, and effectiveness declines with more than 6 participants. Smaller groups allow for more hands-on learning and cognitive engagement. While clinical skills can be taught in larger groups, learners favor smaller groups for debriefing and complex scenarios. Effective curriculum planning should account for available resources, the type of simulation, and the material being taught, with group sizes adjusted to optimize learning outcomes.</p>\",\"PeriodicalId\":45121,\"journal\":{\"name\":\"Journal of Medical Education and Curricular Development\",\"volume\":\"12 \",\"pages\":\"23821205251327287\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-04-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11970070/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medical Education and Curricular Development\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/23821205251327287\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"EDUCATION, SCIENTIFIC DISCIPLINES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Education and Curricular Development","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23821205251327287","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"EDUCATION, SCIENTIFIC DISCIPLINES","Score":null,"Total":0}
Exploring Optimal Group Sizes for Learning in Medical Simulation: A Systematic Review.
Objectives: Simulation is an effective teaching method that improves learner competence and confidence. Optimizing group size balances efficiency without sacrificing efficacy. While simulation technology is widely used in medical education, no standard for learner group size exists. This study investigates the optimal group size for simulation, aiming to identify best practices that maximize efficiency and efficacy in learning environments.
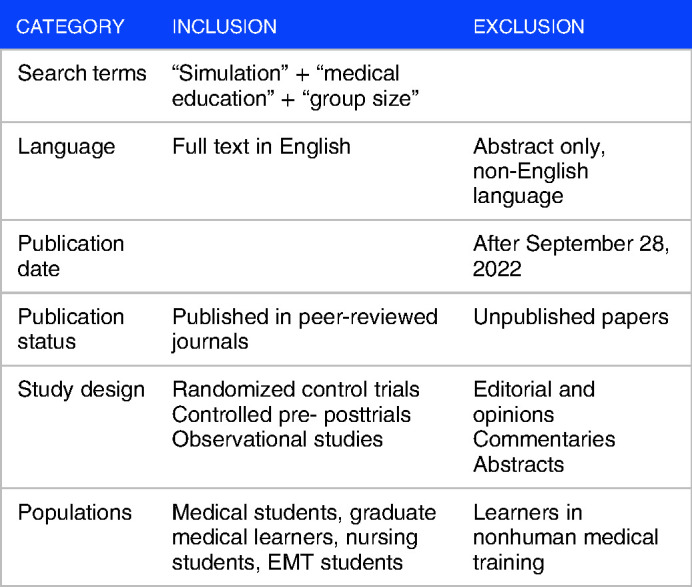
Methods: This systematic review adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. A team of emergency medicine educators screened citations and reviewed relevant full-text articles. Inclusion criteria focused on group sizes with the best outcomes. Quality assessment employed the Medical Education Research Study Quality Instrument approach to evaluate evidence.
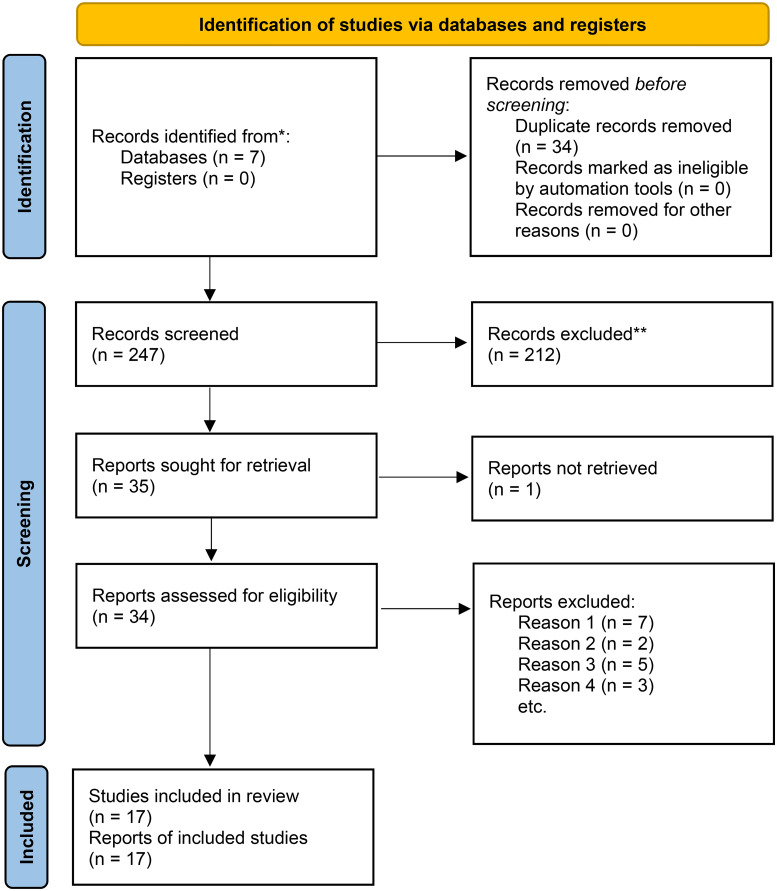
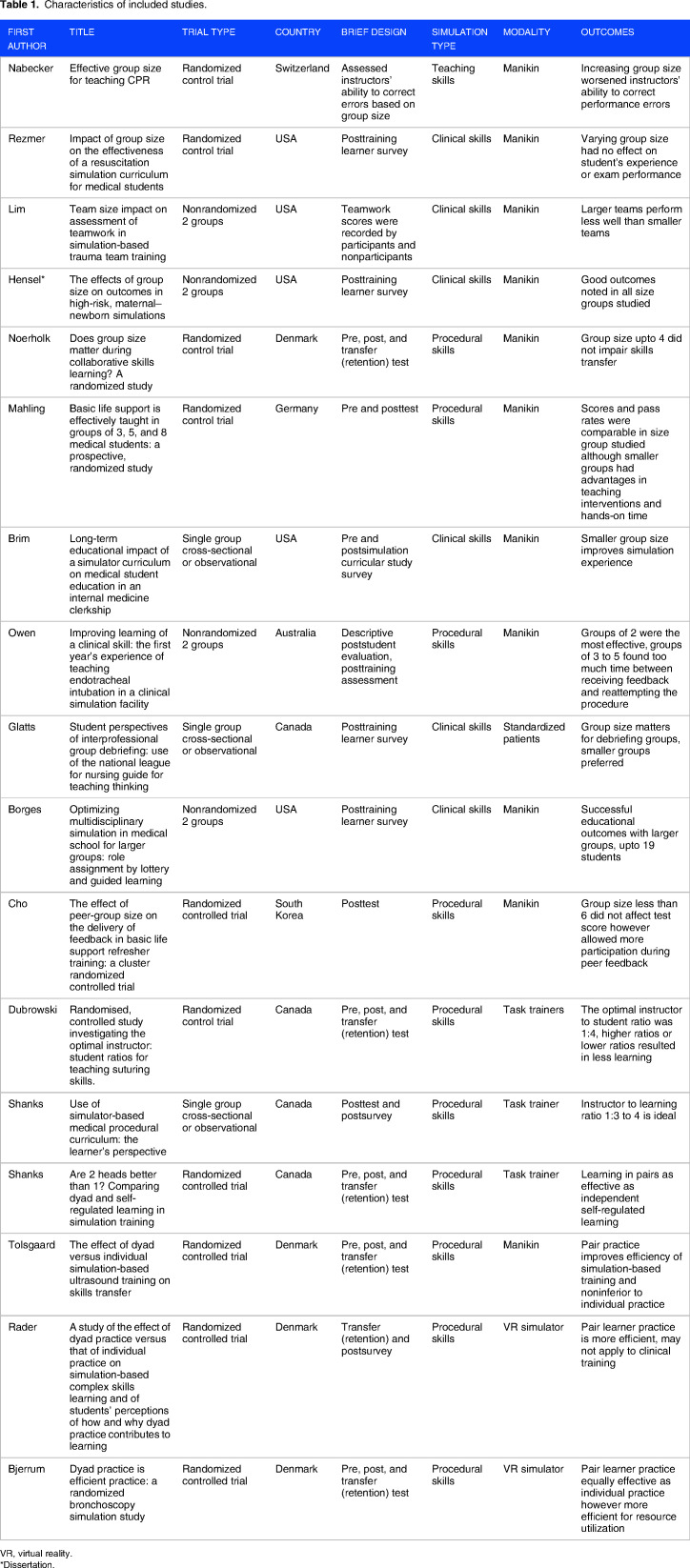
Results: Thirty-four articles were identified; 17 were deemed relevant for full-text review. The studies varied in methods, including prospective and retrospective reviews, mixed methods, and randomized controlled trials. Smaller groups improved outcomes, with an ideal size dependent on learning objectives. Five studies suggested groups of up to 4 learners were optimal, with mixed results on the exact number. One study identified 6 as the ideal group size. Debriefing was effective in larger groups, while procedural skills were best taught in groups of 2 to 4 learners.
Conclusion: This review suggests smaller group sizes are more effective for efficiency, knowledge, and confidence. For procedural skills, groups of 2 to 4 are most effective, and effectiveness declines with more than 6 participants. Smaller groups allow for more hands-on learning and cognitive engagement. While clinical skills can be taught in larger groups, learners favor smaller groups for debriefing and complex scenarios. Effective curriculum planning should account for available resources, the type of simulation, and the material being taught, with group sizes adjusted to optimize learning outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


