{"title":"危重病人早期气管切开术与晚期气管切开术的比较:随机临床试验系统综述与荟萃分析和试验序列分析的总综述。","authors":"Aline Boni, Tiago Antonio Tonietto, Marcos Frata Rihl, Marina Verçoza Viana","doi":"10.1136/bmjresp-2024-002434","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study conducts an umbrella review of systematic reviews and meta-analyses of randomised clinical trials (RCTs) to evaluate the outcomes of early vs late tracheostomy, focusing on potential biases and the coherence of the evidence.</p><p><strong>Data sources: </strong>Searches were conducted in the MEDLINE, Embase, Lilacs and Cochrane Library databases up to November 2024.</p><p><strong>Study selection: </strong>Our analysis included studies meeting the following criteria: Population: patients admitted to intensive care units and receiving mechanical ventilation.</p><p><strong>Intervention: </strong>early tracheostomy, as defined by the respective study.</p><p><strong>Control: </strong>late tracheostomy, as defined by the respective study.</p><p><strong>Primary outcomes: </strong>mortality and incidence of ventilator-associated pneumonia (VAP).</p><p><strong>Study design: </strong>systematic reviews and meta-analysis of RCTs.</p><p><strong>Data extraction: </strong>Two reviewers performed article inclusion, with consensus resolution by a third reviewer in case of disagreement. The quality of studies was assessed using the AMSTAR 2 tool. A random-effects meta-analysis was conducted with an algorithm based on the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) classification DATA SYNTHESIS: Out of 7664 articles identified, 60 articles were considered eligible for full-text reading, and 22 were included in the review. Most studies were rated as critically low quality. Our meta-analysis update with 19 RCTs showed a decrease in VAP (OR 0.65 (0.47 to 0.89), 95% CI; p=0.007) among early tracheostomy patients compared with late tracheostomy patients, but no significant difference in terms of mortality (OR 0.85 (0.70 to 1.03), 95% CI; p=0.09). A trial sequential analysis indicated that the current data are insufficient to reach a definitive conclusion.</p><p><strong>Conclusion: </strong>In summary, despite extensive research on tracheostomy timing and its outcomes, as well as a correlation in our study between early tracheostomy and reduced VAP incidence, evidence remains weak. Besides that, no clear mortality benefits were observed. Further research using a different approach is crucial to identify the specific population that may derive benefits from early tracheostomy.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-04-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11973787/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early versus late tracheostomy in critically ill patients: an umbrella review of systematic reviews of randomised clinical trials with meta-analyses and trial sequential analysis.\",\"authors\":\"Aline Boni, Tiago Antonio Tonietto, Marcos Frata Rihl, Marina Verçoza Viana\",\"doi\":\"10.1136/bmjresp-2024-002434\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study conducts an umbrella review of systematic reviews and meta-analyses of randomised clinical trials (RCTs) to evaluate the outcomes of early vs late tracheostomy, focusing on potential biases and the coherence of the evidence.</p><p><strong>Data sources: </strong>Searches were conducted in the MEDLINE, Embase, Lilacs and Cochrane Library databases up to November 2024.</p><p><strong>Study selection: </strong>Our analysis included studies meeting the following criteria: Population: patients admitted to intensive care units and receiving mechanical ventilation.</p><p><strong>Intervention: </strong>early tracheostomy, as defined by the respective study.</p><p><strong>Control: </strong>late tracheostomy, as defined by the respective study.</p><p><strong>Primary outcomes: </strong>mortality and incidence of ventilator-associated pneumonia (VAP).</p><p><strong>Study design: </strong>systematic reviews and meta-analysis of RCTs.</p><p><strong>Data extraction: </strong>Two reviewers performed article inclusion, with consensus resolution by a third reviewer in case of disagreement. The quality of studies was assessed using the AMSTAR 2 tool. A random-effects meta-analysis was conducted with an algorithm based on the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) classification DATA SYNTHESIS: Out of 7664 articles identified, 60 articles were considered eligible for full-text reading, and 22 were included in the review. Most studies were rated as critically low quality. Our meta-analysis update with 19 RCTs showed a decrease in VAP (OR 0.65 (0.47 to 0.89), 95% CI; p=0.007) among early tracheostomy patients compared with late tracheostomy patients, but no significant difference in terms of mortality (OR 0.85 (0.70 to 1.03), 95% CI; p=0.09). A trial sequential analysis indicated that the current data are insufficient to reach a definitive conclusion.</p><p><strong>Conclusion: </strong>In summary, despite extensive research on tracheostomy timing and its outcomes, as well as a correlation in our study between early tracheostomy and reduced VAP incidence, evidence remains weak. Besides that, no clear mortality benefits were observed. Further research using a different approach is crucial to identify the specific population that may derive benefits from early tracheostomy.</p>\",\"PeriodicalId\":9048,\"journal\":{\"name\":\"BMJ Open Respiratory Research\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-04-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11973787/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjresp-2024-002434\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002434","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Early versus late tracheostomy in critically ill patients: an umbrella review of systematic reviews of randomised clinical trials with meta-analyses and trial sequential analysis.
Objective: This study conducts an umbrella review of systematic reviews and meta-analyses of randomised clinical trials (RCTs) to evaluate the outcomes of early vs late tracheostomy, focusing on potential biases and the coherence of the evidence.
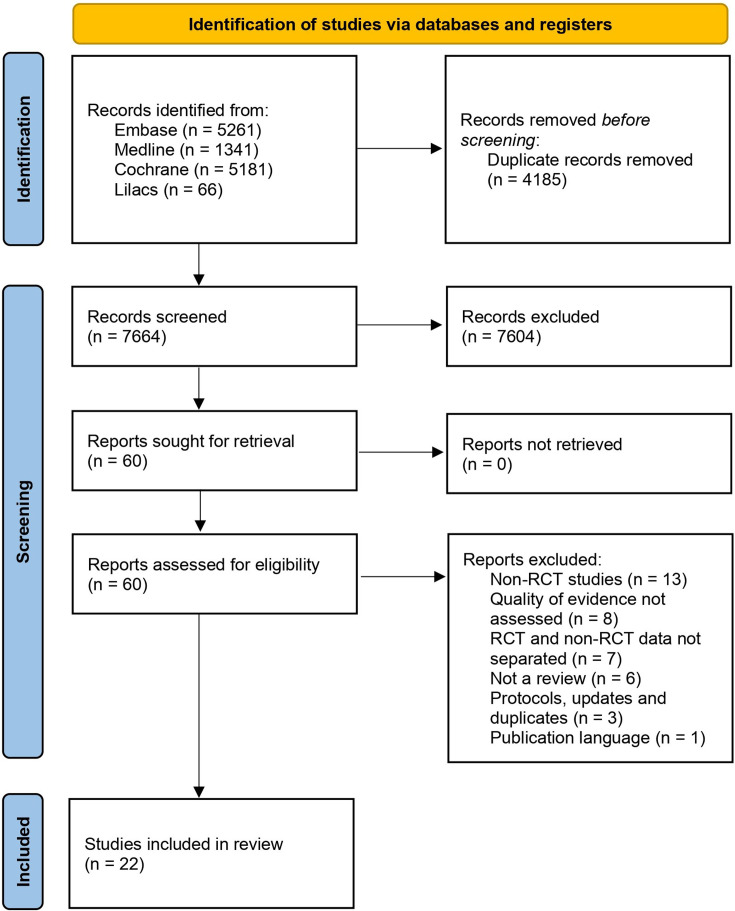
Data sources: Searches were conducted in the MEDLINE, Embase, Lilacs and Cochrane Library databases up to November 2024.
Study selection: Our analysis included studies meeting the following criteria: Population: patients admitted to intensive care units and receiving mechanical ventilation.
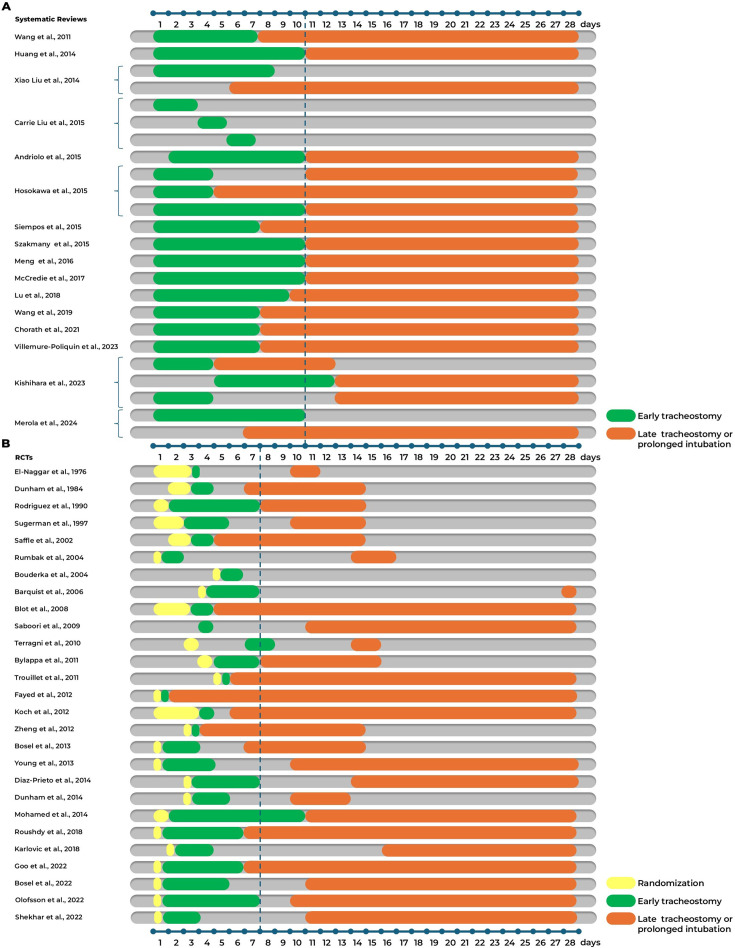
Intervention: early tracheostomy, as defined by the respective study.
Control: late tracheostomy, as defined by the respective study.
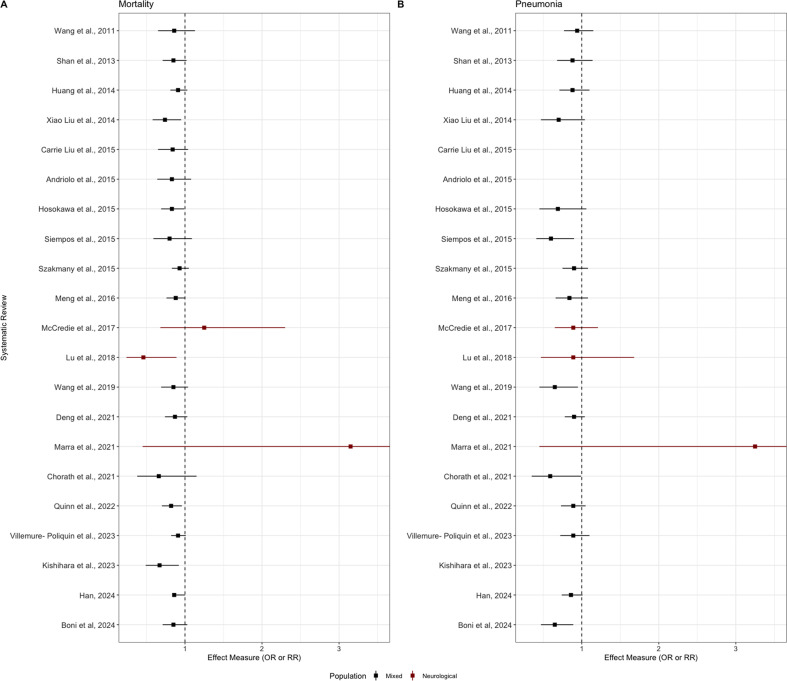
Primary outcomes: mortality and incidence of ventilator-associated pneumonia (VAP).
Study design: systematic reviews and meta-analysis of RCTs.
Data extraction: Two reviewers performed article inclusion, with consensus resolution by a third reviewer in case of disagreement. The quality of studies was assessed using the AMSTAR 2 tool. A random-effects meta-analysis was conducted with an algorithm based on the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) classification DATA SYNTHESIS: Out of 7664 articles identified, 60 articles were considered eligible for full-text reading, and 22 were included in the review. Most studies were rated as critically low quality. Our meta-analysis update with 19 RCTs showed a decrease in VAP (OR 0.65 (0.47 to 0.89), 95% CI; p=0.007) among early tracheostomy patients compared with late tracheostomy patients, but no significant difference in terms of mortality (OR 0.85 (0.70 to 1.03), 95% CI; p=0.09). A trial sequential analysis indicated that the current data are insufficient to reach a definitive conclusion.
Conclusion: In summary, despite extensive research on tracheostomy timing and its outcomes, as well as a correlation in our study between early tracheostomy and reduced VAP incidence, evidence remains weak. Besides that, no clear mortality benefits were observed. Further research using a different approach is crucial to identify the specific population that may derive benefits from early tracheostomy.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


