{"title":"骨折或吸脂引起的脂肪栓塞综合征:9例回顾性病例系列。","authors":"Xuexin Yan, Siyao Wu, Wen Zeng, Jinliang Kong","doi":"10.1080/07853890.2024.2447427","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fat embolism syndrome (FES) is a rare and potentially fatal complication commonly observed after liposuction or fractures. Patients with FES often have an acute onset and a rapid course of disease. However, there is a paucity of research summarizing the clinical features of FES caused by simultaneous fracture or liposuction.</p><p><strong>Methods: </strong>A comprehensive analysis was conducted to enhance understanding of patients with FES associated with either fractures or liposuction procedures.</p><p><strong>Results: </strong>Nine patients who were diagnosed with FES were included in our study, of whom two were male. Six patients underwent liposuction, while three sustained multiple orthopaedic fractures. Postoperative liposuction complications occurred rapidly (average 1.8 h) after surgery, whereas patients with fractures experienced symptoms approximately 24 h after injury. All patients presented with respiratory insufficiency, six patients had cerebral involvement, and four patients had petechial haemorrhage. Laboratory tests revealed that six patients had leucocytosis, five patients had elevated neutrophil counts and eight patients had increased D-dimer concentrations. Seven patients exhibited decreased partial pressure of oxygen (7/9), six presented with decreased haemoglobin (6/9) and four had thrombocytopenia (4/9). Chest computed tomography (CT) revealed pneumonia with symmetrically diffuse ground glass opacities and patchy exudates in both lungs, which are the most common radiographic findings (8/9). Brain CT of five patients revealed multiple cerebral infarctions, and CT angiograms of the head and neck demonstrated corresponding vessel occlusions in one patient. All patients received supportive care, including six who received noninvasive ventilation and three who received mechanical ventilation. Additionally, seven patients were treated with corticosteroids. Eight patients survived, while one died of sustained cerebral embolism and ischaemia during treatment.</p><p><strong>Conclusions: </strong>A patient's medical history is critical for the diagnosis of FES. Early diagnosis and timely treatment can reduce mortality, while supportive care is important, and corticosteroid therapy may be effective for early treatment.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2447427"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11703124/pdf/","citationCount":"0","resultStr":"{\"title\":\"Fat embolism syndrome caused by fracture or liposuction: a retrospective case series of nine patients.\",\"authors\":\"Xuexin Yan, Siyao Wu, Wen Zeng, Jinliang Kong\",\"doi\":\"10.1080/07853890.2024.2447427\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Fat embolism syndrome (FES) is a rare and potentially fatal complication commonly observed after liposuction or fractures. Patients with FES often have an acute onset and a rapid course of disease. However, there is a paucity of research summarizing the clinical features of FES caused by simultaneous fracture or liposuction.</p><p><strong>Methods: </strong>A comprehensive analysis was conducted to enhance understanding of patients with FES associated with either fractures or liposuction procedures.</p><p><strong>Results: </strong>Nine patients who were diagnosed with FES were included in our study, of whom two were male. Six patients underwent liposuction, while three sustained multiple orthopaedic fractures. Postoperative liposuction complications occurred rapidly (average 1.8 h) after surgery, whereas patients with fractures experienced symptoms approximately 24 h after injury. All patients presented with respiratory insufficiency, six patients had cerebral involvement, and four patients had petechial haemorrhage. Laboratory tests revealed that six patients had leucocytosis, five patients had elevated neutrophil counts and eight patients had increased D-dimer concentrations. Seven patients exhibited decreased partial pressure of oxygen (7/9), six presented with decreased haemoglobin (6/9) and four had thrombocytopenia (4/9). Chest computed tomography (CT) revealed pneumonia with symmetrically diffuse ground glass opacities and patchy exudates in both lungs, which are the most common radiographic findings (8/9). Brain CT of five patients revealed multiple cerebral infarctions, and CT angiograms of the head and neck demonstrated corresponding vessel occlusions in one patient. All patients received supportive care, including six who received noninvasive ventilation and three who received mechanical ventilation. Additionally, seven patients were treated with corticosteroids. Eight patients survived, while one died of sustained cerebral embolism and ischaemia during treatment.</p><p><strong>Conclusions: </strong>A patient's medical history is critical for the diagnosis of FES. Early diagnosis and timely treatment can reduce mortality, while supportive care is important, and corticosteroid therapy may be effective for early treatment.</p>\",\"PeriodicalId\":93874,\"journal\":{\"name\":\"Annals of medicine\",\"volume\":\"57 1\",\"pages\":\"2447427\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2025-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11703124/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/07853890.2024.2447427\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2024.2447427","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Fat embolism syndrome caused by fracture or liposuction: a retrospective case series of nine patients.
Background: Fat embolism syndrome (FES) is a rare and potentially fatal complication commonly observed after liposuction or fractures. Patients with FES often have an acute onset and a rapid course of disease. However, there is a paucity of research summarizing the clinical features of FES caused by simultaneous fracture or liposuction.
Methods: A comprehensive analysis was conducted to enhance understanding of patients with FES associated with either fractures or liposuction procedures.
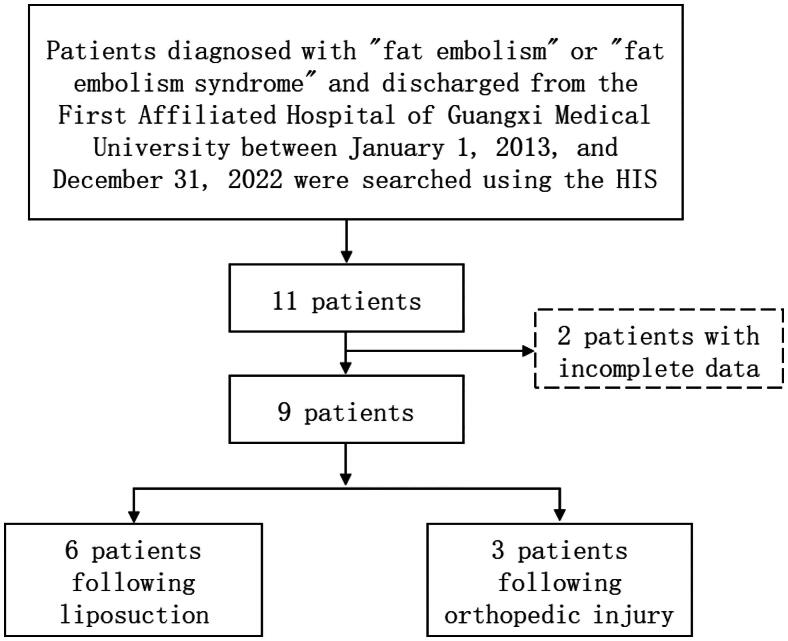
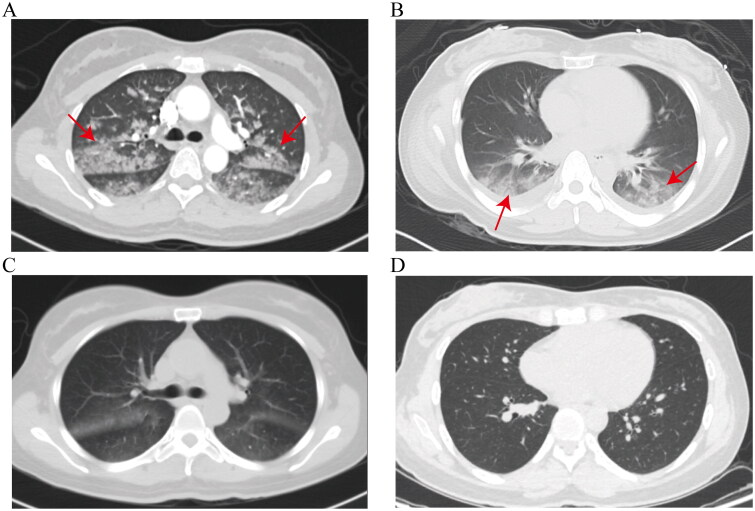
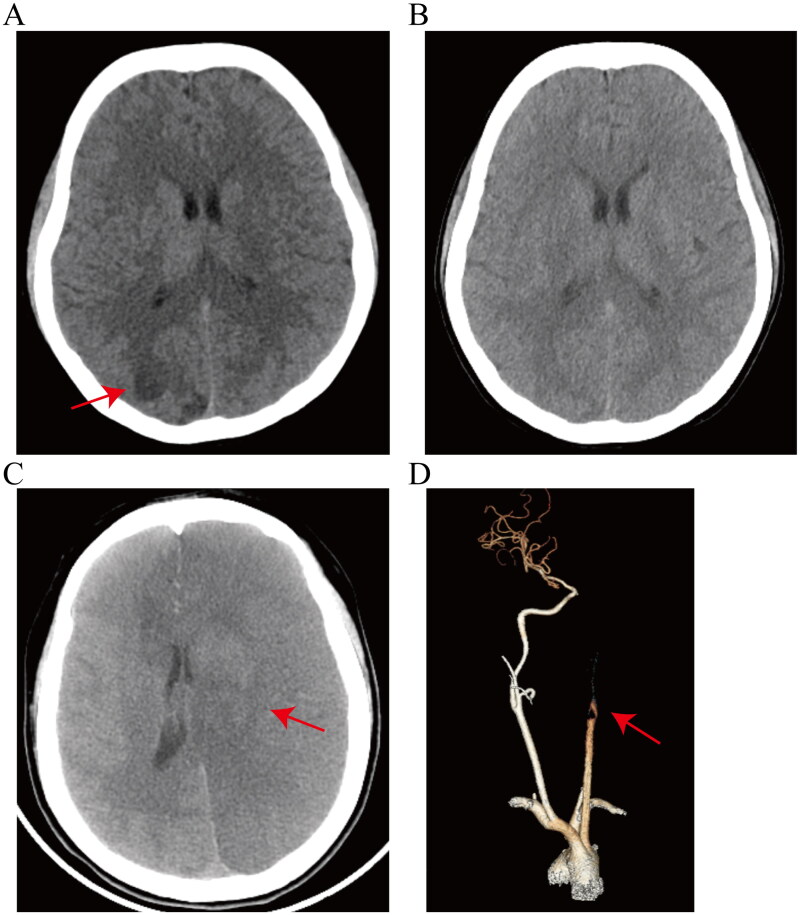
Results: Nine patients who were diagnosed with FES were included in our study, of whom two were male. Six patients underwent liposuction, while three sustained multiple orthopaedic fractures. Postoperative liposuction complications occurred rapidly (average 1.8 h) after surgery, whereas patients with fractures experienced symptoms approximately 24 h after injury. All patients presented with respiratory insufficiency, six patients had cerebral involvement, and four patients had petechial haemorrhage. Laboratory tests revealed that six patients had leucocytosis, five patients had elevated neutrophil counts and eight patients had increased D-dimer concentrations. Seven patients exhibited decreased partial pressure of oxygen (7/9), six presented with decreased haemoglobin (6/9) and four had thrombocytopenia (4/9). Chest computed tomography (CT) revealed pneumonia with symmetrically diffuse ground glass opacities and patchy exudates in both lungs, which are the most common radiographic findings (8/9). Brain CT of five patients revealed multiple cerebral infarctions, and CT angiograms of the head and neck demonstrated corresponding vessel occlusions in one patient. All patients received supportive care, including six who received noninvasive ventilation and three who received mechanical ventilation. Additionally, seven patients were treated with corticosteroids. Eight patients survived, while one died of sustained cerebral embolism and ischaemia during treatment.
Conclusions: A patient's medical history is critical for the diagnosis of FES. Early diagnosis and timely treatment can reduce mortality, while supportive care is important, and corticosteroid therapy may be effective for early treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


