Samuel G S Gunning, John Graby, Yashesh Mody, Pia F P Charters, Tim A Burnett, David Murphy, Ali Khavandi, Jonathan C L Rodrigues
{"title":"常规非门控胸部CT对主动脉瓣钙化的视觉分级预测预后并改变处理方法。","authors":"Samuel G S Gunning, John Graby, Yashesh Mody, Pia F P Charters, Tim A Burnett, David Murphy, Ali Khavandi, Jonathan C L Rodrigues","doi":"10.1007/s00330-025-11553-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>BSCI/BSTI guidelines recommend reporting aortic valve calcification (AVC) on all chest CTs regardless of indication. We assessed AVC frequency, severity, and association with aortic stenosis (AS) on echocardiography and its prognostic implications.</p><p><strong>Methods: </strong>Retrospective, single-centre analysis of consecutive chest CTs (January-December 2015) for 200 patients per age group (< 40, 40-49, 50-59, 60-69, 70-79, 80-89, ≥ 90) performed for medical, surgical, and oncological indications. CTs were re-reviewed for the presence and graded severity of AVC and coronary artery calcification (CAC). Corresponding echocardiography reports (within 5 years) reviewed for AS. Comorbidities and clinical outcomes were recorded.</p><p><strong>Results: </strong>One thousand three hundred seventy-seven patients were included (mean age 64 ± 20 years, 55% female). AVC was present in 25% (350/1377) and was more prevalent in males (p < 0.001). Frequency and severity increased with age (p < 0.001). 38% (524/1377) had an echocardiogram (median inter-test interval 4.3 months [IQR 0.4-17.5]). Sixteen per cent (29/178) with AVC had AS of any severity (8% [15/178] mild; 8% [14/178] moderate; 0% [0/178] severe). Sensitivity and specificity for AVC predicting AS were 91% and 70%, respectively. Extrapolating findings, 8% of individuals with AVC and without an echocardiogram may have undiagnosed AS. All-cause mortality occurred in 53% (734/1377), which AVC predicted independently of CAC and age (p < 0.001). Adjusting for confounders, severe AVC predicted all-cause mortality (HR 1.56 [1.10-2.22], p = 0.013).</p><p><strong>Conclusions: </strong>AVC identified AS in 16% of patients. Additionally, severe AVC is an independent predictor of all-cause mortality in multivariable analysis. Validation in a prospective cohort is required to inform clinical practice guidelines.</p><p><strong>Key points: </strong>Question New guidelines recommend reporting AVC on all non-gated chest CTs, the prognostic and clinical relevance of which is uncertain. Findings There are associations between visually quantified AVC, AS on echocardiography, and all-cause mortality in an unselected population referred for routine chest CT. Clinical relevance These results support the reporting of all severities of AVC, especially severe AVC, as a prognostic marker in all age groups. The clinical implications require further clarification in a prospective cohort.</p>","PeriodicalId":12076,"journal":{"name":"European Radiology","volume":" ","pages":"6291-6301"},"PeriodicalIF":4.7000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417276/pdf/","citationCount":"0","resultStr":"{\"title\":\"Visual ordinal grading of aortic valve calcification on routine non-gated chest CT predicts prognosis and alters management.\",\"authors\":\"Samuel G S Gunning, John Graby, Yashesh Mody, Pia F P Charters, Tim A Burnett, David Murphy, Ali Khavandi, Jonathan C L Rodrigues\",\"doi\":\"10.1007/s00330-025-11553-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>BSCI/BSTI guidelines recommend reporting aortic valve calcification (AVC) on all chest CTs regardless of indication. We assessed AVC frequency, severity, and association with aortic stenosis (AS) on echocardiography and its prognostic implications.</p><p><strong>Methods: </strong>Retrospective, single-centre analysis of consecutive chest CTs (January-December 2015) for 200 patients per age group (< 40, 40-49, 50-59, 60-69, 70-79, 80-89, ≥ 90) performed for medical, surgical, and oncological indications. CTs were re-reviewed for the presence and graded severity of AVC and coronary artery calcification (CAC). Corresponding echocardiography reports (within 5 years) reviewed for AS. Comorbidities and clinical outcomes were recorded.</p><p><strong>Results: </strong>One thousand three hundred seventy-seven patients were included (mean age 64 ± 20 years, 55% female). AVC was present in 25% (350/1377) and was more prevalent in males (p < 0.001). Frequency and severity increased with age (p < 0.001). 38% (524/1377) had an echocardiogram (median inter-test interval 4.3 months [IQR 0.4-17.5]). Sixteen per cent (29/178) with AVC had AS of any severity (8% [15/178] mild; 8% [14/178] moderate; 0% [0/178] severe). Sensitivity and specificity for AVC predicting AS were 91% and 70%, respectively. Extrapolating findings, 8% of individuals with AVC and without an echocardiogram may have undiagnosed AS. All-cause mortality occurred in 53% (734/1377), which AVC predicted independently of CAC and age (p < 0.001). Adjusting for confounders, severe AVC predicted all-cause mortality (HR 1.56 [1.10-2.22], p = 0.013).</p><p><strong>Conclusions: </strong>AVC identified AS in 16% of patients. Additionally, severe AVC is an independent predictor of all-cause mortality in multivariable analysis. Validation in a prospective cohort is required to inform clinical practice guidelines.</p><p><strong>Key points: </strong>Question New guidelines recommend reporting AVC on all non-gated chest CTs, the prognostic and clinical relevance of which is uncertain. Findings There are associations between visually quantified AVC, AS on echocardiography, and all-cause mortality in an unselected population referred for routine chest CT. Clinical relevance These results support the reporting of all severities of AVC, especially severe AVC, as a prognostic marker in all age groups. The clinical implications require further clarification in a prospective cohort.</p>\",\"PeriodicalId\":12076,\"journal\":{\"name\":\"European Radiology\",\"volume\":\" \",\"pages\":\"6291-6301\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417276/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Radiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00330-025-11553-w\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00330-025-11553-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/2 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Visual ordinal grading of aortic valve calcification on routine non-gated chest CT predicts prognosis and alters management.
Objective: BSCI/BSTI guidelines recommend reporting aortic valve calcification (AVC) on all chest CTs regardless of indication. We assessed AVC frequency, severity, and association with aortic stenosis (AS) on echocardiography and its prognostic implications.
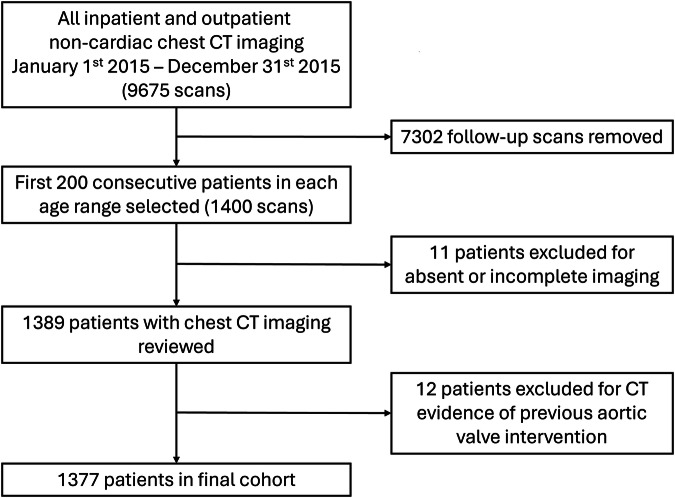
Methods: Retrospective, single-centre analysis of consecutive chest CTs (January-December 2015) for 200 patients per age group (< 40, 40-49, 50-59, 60-69, 70-79, 80-89, ≥ 90) performed for medical, surgical, and oncological indications. CTs were re-reviewed for the presence and graded severity of AVC and coronary artery calcification (CAC). Corresponding echocardiography reports (within 5 years) reviewed for AS. Comorbidities and clinical outcomes were recorded.
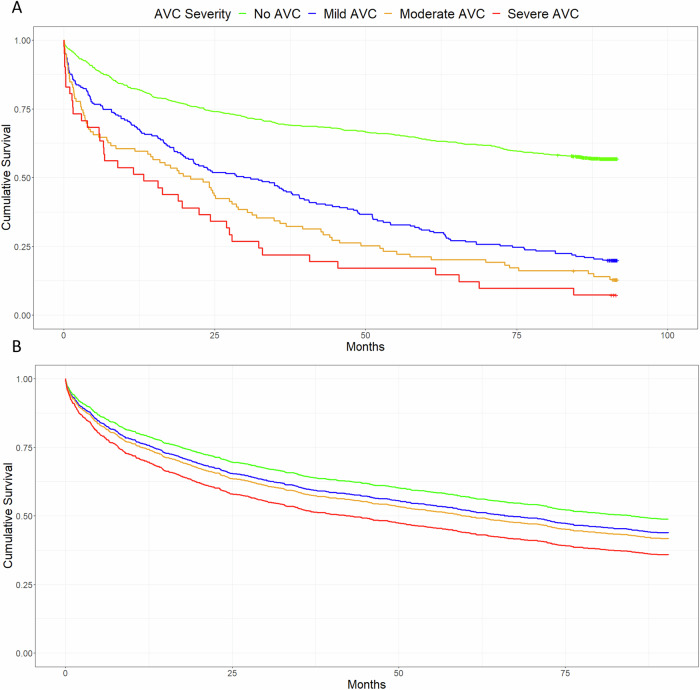
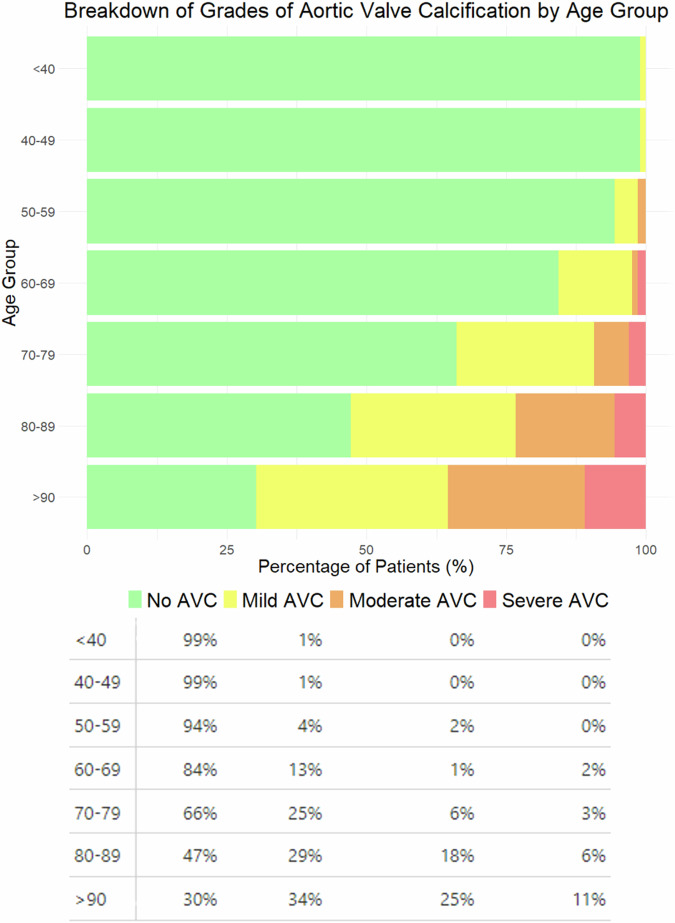
Results: One thousand three hundred seventy-seven patients were included (mean age 64 ± 20 years, 55% female). AVC was present in 25% (350/1377) and was more prevalent in males (p < 0.001). Frequency and severity increased with age (p < 0.001). 38% (524/1377) had an echocardiogram (median inter-test interval 4.3 months [IQR 0.4-17.5]). Sixteen per cent (29/178) with AVC had AS of any severity (8% [15/178] mild; 8% [14/178] moderate; 0% [0/178] severe). Sensitivity and specificity for AVC predicting AS were 91% and 70%, respectively. Extrapolating findings, 8% of individuals with AVC and without an echocardiogram may have undiagnosed AS. All-cause mortality occurred in 53% (734/1377), which AVC predicted independently of CAC and age (p < 0.001). Adjusting for confounders, severe AVC predicted all-cause mortality (HR 1.56 [1.10-2.22], p = 0.013).
Conclusions: AVC identified AS in 16% of patients. Additionally, severe AVC is an independent predictor of all-cause mortality in multivariable analysis. Validation in a prospective cohort is required to inform clinical practice guidelines.
Key points: Question New guidelines recommend reporting AVC on all non-gated chest CTs, the prognostic and clinical relevance of which is uncertain. Findings There are associations between visually quantified AVC, AS on echocardiography, and all-cause mortality in an unselected population referred for routine chest CT. Clinical relevance These results support the reporting of all severities of AVC, especially severe AVC, as a prognostic marker in all age groups. The clinical implications require further clarification in a prospective cohort.
期刊介绍:
European Radiology (ER) continuously updates scientific knowledge in radiology by publication of strong original articles and state-of-the-art reviews written by leading radiologists. A well balanced combination of review articles, original papers, short communications from European radiological congresses and information on society matters makes ER an indispensable source for current information in this field.
This is the Journal of the European Society of Radiology, and the official journal of a number of societies.
From 2004-2008 supplements to European Radiology were published under its companion, European Radiology Supplements, ISSN 1613-3749.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


