Ahmad Mustafa, Chapman Wei, Michael Cinelli, Shahkar Khan, Danyal Khan, Frank Tamburrino, Gregory Maniatis, Jonathan Spagnola
{"title":"球囊瓣膜成形术及经导管股动脉旁路主动脉瓣置换术:1例报告及文献复习。","authors":"Ahmad Mustafa, Chapman Wei, Michael Cinelli, Shahkar Khan, Danyal Khan, Frank Tamburrino, Gregory Maniatis, Jonathan Spagnola","doi":"10.4330/wjc.v17.i3.101709","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transcatheter aortic valve replacement (TAVR) can be performed through multiple access sites with the preferred approach being transfemoral. In patients with severe peripheral arterial disease and previous grafts, the safety of transfemoral access <i>via</i> direct graft puncture, especially when performed twice within a short period, remains unclear compared to alternative access methods. We present a case demonstrating the safety and efficacy of direct graft puncture for transfemoral access during balloon aortic valvuloplasty (BAV) and TAVR.</p><p><strong>Case summary: </strong>An 82-year-old man presented with dyspnea on exertion. Echocardiogram was significant for severe aortic stenosis. Following a heart team discussion, the patient was scheduled for a balloon valvuloplasty followed by staged TAVR. Based on pre-TAVR computed tomography angiogram, the aortobifemoral graft was deemed as an appropriate access site. Micropuncture needle was used to access the right femoral artery graft, and the sheath was upscaled to 10 Fr. He underwent successful intervention to ostial left anterior descending and left circumflex arteries, and BAV with 22 mm Vida BAV balloon. Hemostasis was achieved using Perclose. For TAVR, an 8 Fr sheath was inserted <i>via</i> the right femoral bypass graft. The arteriotomy was pre-closed with two Perclose ProGlides and access was upsized to 18F Gore DrySeal. A 5Fr sheath was used for left femoral bypass graft access. Patient underwent successful TAVR with 29 mm CoreValve. Hemostasis was successfully achieved using 2 Perclose for right access site and one Perclose for left side with no postoperative bleeding complications.</p><p><strong>Conclusion: </strong>BAV and TAVR are feasible and safe through a direct puncture of the aortofemoral bypass graft with successful hemostasis using Perclose.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 3","pages":"101709"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11947954/pdf/","citationCount":"0","resultStr":"{\"title\":\"Balloon valvuloplasty and transcatheter aortic valve replacement <i>via</i> aortofemoral bypass grafts: A case report and review of literature.\",\"authors\":\"Ahmad Mustafa, Chapman Wei, Michael Cinelli, Shahkar Khan, Danyal Khan, Frank Tamburrino, Gregory Maniatis, Jonathan Spagnola\",\"doi\":\"10.4330/wjc.v17.i3.101709\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Transcatheter aortic valve replacement (TAVR) can be performed through multiple access sites with the preferred approach being transfemoral. In patients with severe peripheral arterial disease and previous grafts, the safety of transfemoral access <i>via</i> direct graft puncture, especially when performed twice within a short period, remains unclear compared to alternative access methods. We present a case demonstrating the safety and efficacy of direct graft puncture for transfemoral access during balloon aortic valvuloplasty (BAV) and TAVR.</p><p><strong>Case summary: </strong>An 82-year-old man presented with dyspnea on exertion. Echocardiogram was significant for severe aortic stenosis. Following a heart team discussion, the patient was scheduled for a balloon valvuloplasty followed by staged TAVR. Based on pre-TAVR computed tomography angiogram, the aortobifemoral graft was deemed as an appropriate access site. Micropuncture needle was used to access the right femoral artery graft, and the sheath was upscaled to 10 Fr. He underwent successful intervention to ostial left anterior descending and left circumflex arteries, and BAV with 22 mm Vida BAV balloon. Hemostasis was achieved using Perclose. For TAVR, an 8 Fr sheath was inserted <i>via</i> the right femoral bypass graft. The arteriotomy was pre-closed with two Perclose ProGlides and access was upsized to 18F Gore DrySeal. A 5Fr sheath was used for left femoral bypass graft access. Patient underwent successful TAVR with 29 mm CoreValve. Hemostasis was successfully achieved using 2 Perclose for right access site and one Perclose for left side with no postoperative bleeding complications.</p><p><strong>Conclusion: </strong>BAV and TAVR are feasible and safe through a direct puncture of the aortofemoral bypass graft with successful hemostasis using Perclose.</p>\",\"PeriodicalId\":23800,\"journal\":{\"name\":\"World Journal of Cardiology\",\"volume\":\"17 3\",\"pages\":\"101709\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-03-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11947954/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4330/wjc.v17.i3.101709\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i3.101709","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:经导管主动脉瓣置换术(TAVR)可以通过多个通路进行,首选的途径是经股。在有严重外周动脉疾病和既往移植物的患者中,与其他进入方法相比,通过直接移植物穿刺经股进入的安全性,特别是在短时间内进行两次时,仍不清楚。我们报告了一个病例,证明了在球囊主动脉瓣成形术(BAV)和TAVR期间,直接移植物穿刺经股通道的安全性和有效性。病例总结:一名82岁男性在用力时出现呼吸困难。超声心动图对严重主动脉狭窄有显著意义。在心脏小组讨论后,患者被安排进行球囊瓣膜成形术,随后进行分阶段TAVR。基于tavr前的计算机断层血管造影,认为主动脉股动脉移植物是一个合适的进入部位。显微穿刺针进入右股动脉移植物,鞘层扩大至10 Fr。患者成功介入左前降动脉和左旋动脉,并使用22 mm Vida BAV球囊进行BAV。使用Perclose止血。对于TAVR,通过右股旁路移植术插入8fr鞘。用两个Perclose ProGlides预封闭动脉切开术,并将通道放大至18F Gore DrySeal。5Fr护套用于左股旁路移植术。患者成功接受了29 mm CoreValve的TAVR。右侧通路2次Perclose,左侧通路1次Perclose止血成功,无术后出血并发症。结论:经Perclose止血成功,直接穿刺股主动脉旁路移植术行BAV和TAVR是可行和安全的。
Balloon valvuloplasty and transcatheter aortic valve replacement via aortofemoral bypass grafts: A case report and review of literature.
Background: Transcatheter aortic valve replacement (TAVR) can be performed through multiple access sites with the preferred approach being transfemoral. In patients with severe peripheral arterial disease and previous grafts, the safety of transfemoral access via direct graft puncture, especially when performed twice within a short period, remains unclear compared to alternative access methods. We present a case demonstrating the safety and efficacy of direct graft puncture for transfemoral access during balloon aortic valvuloplasty (BAV) and TAVR.
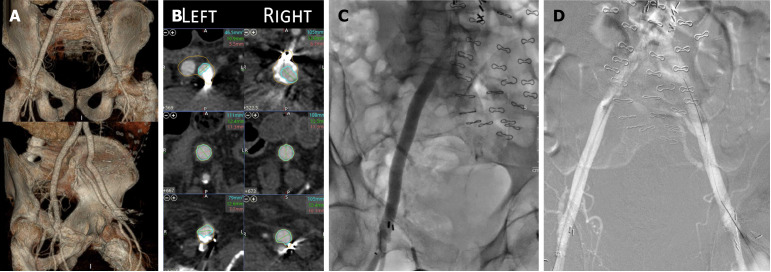
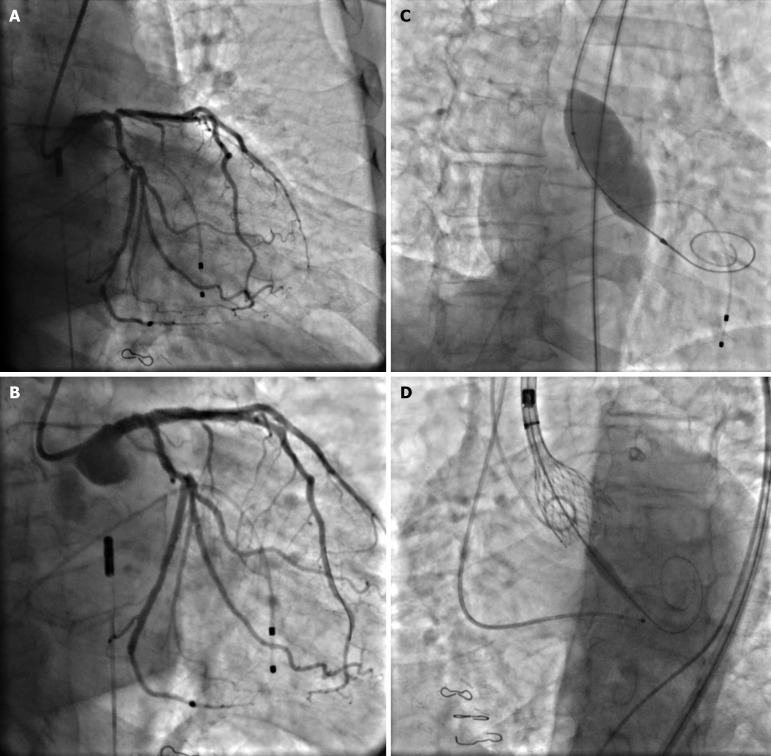
Case summary: An 82-year-old man presented with dyspnea on exertion. Echocardiogram was significant for severe aortic stenosis. Following a heart team discussion, the patient was scheduled for a balloon valvuloplasty followed by staged TAVR. Based on pre-TAVR computed tomography angiogram, the aortobifemoral graft was deemed as an appropriate access site. Micropuncture needle was used to access the right femoral artery graft, and the sheath was upscaled to 10 Fr. He underwent successful intervention to ostial left anterior descending and left circumflex arteries, and BAV with 22 mm Vida BAV balloon. Hemostasis was achieved using Perclose. For TAVR, an 8 Fr sheath was inserted via the right femoral bypass graft. The arteriotomy was pre-closed with two Perclose ProGlides and access was upsized to 18F Gore DrySeal. A 5Fr sheath was used for left femoral bypass graft access. Patient underwent successful TAVR with 29 mm CoreValve. Hemostasis was successfully achieved using 2 Perclose for right access site and one Perclose for left side with no postoperative bleeding complications.
Conclusion: BAV and TAVR are feasible and safe through a direct puncture of the aortofemoral bypass graft with successful hemostasis using Perclose.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


