{"title":"免疫检查点抑制剂和晚期非小细胞肺癌心肌炎:一项全国性队列研究。","authors":"Fu-Xiao Li, Jia-Xin Cai, Ji-Bin Li, Kong-Jia Luo, Shi-Yu Wang, Wei-Hua Meng, Feng Sha, Zhi-Rong Yang, Allan Hackshaw, Jin-Ling Tang","doi":"10.1186/s40959-025-00325-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Evidence suggests immune checkpoint inhibitor (ICI) can increase the risk of myocarditis. We investigated it in a large national cohort in China.</p><p><strong>Methods: </strong>Patients with stage IIIB-IV non-small cell lung cancer (NSCLC) using data from China's National Anti-Tumor Drug Surveillance System between January 2013 and December 2021. Exposure density sampling was applied to control for immortal time bias. Multivariate Cox regression with time-dependent exposures was used to examine the association between ICI therapy and the incidence of myocarditis while controlling for confounders.</p><p><strong>Results: </strong>55,219 patients were included. The median age was 61 years, and 62% were males. At one-year follow-up (median 335 days), there were 26 cases of myocarditis among ICI users and 28 cases among ICI non-users (a cumulative incidence of 4.8 and 0.6 per 1000 person-years respectively). The adjusted hazard ratio (HR) of myocarditis for ICI users was 7.41 (95% confidence interval [CI]: 3.29-16.67). For programmed cell death protein 1 inhibitor users the HR was 8.39 (95% CI: 3.56-19.77). No significant interactions were observed in subgroup analysis. The results remained unchanged in sensitivity analyses.</p><p><strong>Conclusions: </strong>This study showed that ICI therapy considerably increased the risk of myocarditis, supporting the need for closer monitoring of patients receiving ICI therapies.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"33"},"PeriodicalIF":3.2000,"publicationDate":"2025-03-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11956456/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immune checkpoint inhibitors and myocarditis in advanced non-small cell lung cancer: a nationwide cohort study.\",\"authors\":\"Fu-Xiao Li, Jia-Xin Cai, Ji-Bin Li, Kong-Jia Luo, Shi-Yu Wang, Wei-Hua Meng, Feng Sha, Zhi-Rong Yang, Allan Hackshaw, Jin-Ling Tang\",\"doi\":\"10.1186/s40959-025-00325-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Evidence suggests immune checkpoint inhibitor (ICI) can increase the risk of myocarditis. We investigated it in a large national cohort in China.</p><p><strong>Methods: </strong>Patients with stage IIIB-IV non-small cell lung cancer (NSCLC) using data from China's National Anti-Tumor Drug Surveillance System between January 2013 and December 2021. Exposure density sampling was applied to control for immortal time bias. Multivariate Cox regression with time-dependent exposures was used to examine the association between ICI therapy and the incidence of myocarditis while controlling for confounders.</p><p><strong>Results: </strong>55,219 patients were included. The median age was 61 years, and 62% were males. At one-year follow-up (median 335 days), there were 26 cases of myocarditis among ICI users and 28 cases among ICI non-users (a cumulative incidence of 4.8 and 0.6 per 1000 person-years respectively). The adjusted hazard ratio (HR) of myocarditis for ICI users was 7.41 (95% confidence interval [CI]: 3.29-16.67). For programmed cell death protein 1 inhibitor users the HR was 8.39 (95% CI: 3.56-19.77). No significant interactions were observed in subgroup analysis. The results remained unchanged in sensitivity analyses.</p><p><strong>Conclusions: </strong>This study showed that ICI therapy considerably increased the risk of myocarditis, supporting the need for closer monitoring of patients receiving ICI therapies.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"11 1\",\"pages\":\"33\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-03-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11956456/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-025-00325-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00325-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Immune checkpoint inhibitors and myocarditis in advanced non-small cell lung cancer: a nationwide cohort study.
Objective: Evidence suggests immune checkpoint inhibitor (ICI) can increase the risk of myocarditis. We investigated it in a large national cohort in China.
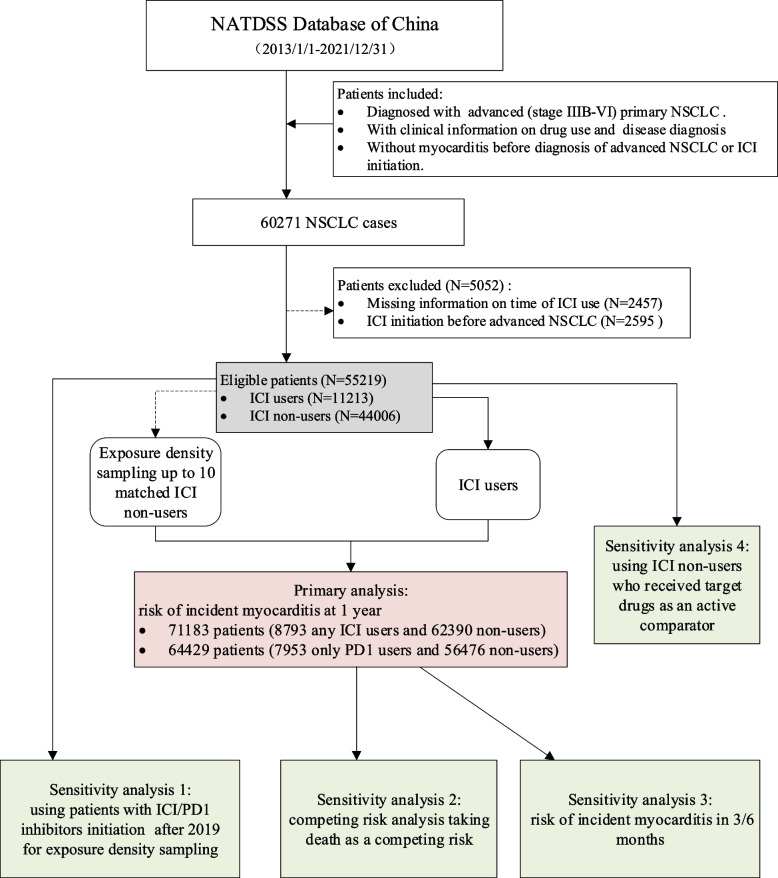
Methods: Patients with stage IIIB-IV non-small cell lung cancer (NSCLC) using data from China's National Anti-Tumor Drug Surveillance System between January 2013 and December 2021. Exposure density sampling was applied to control for immortal time bias. Multivariate Cox regression with time-dependent exposures was used to examine the association between ICI therapy and the incidence of myocarditis while controlling for confounders.
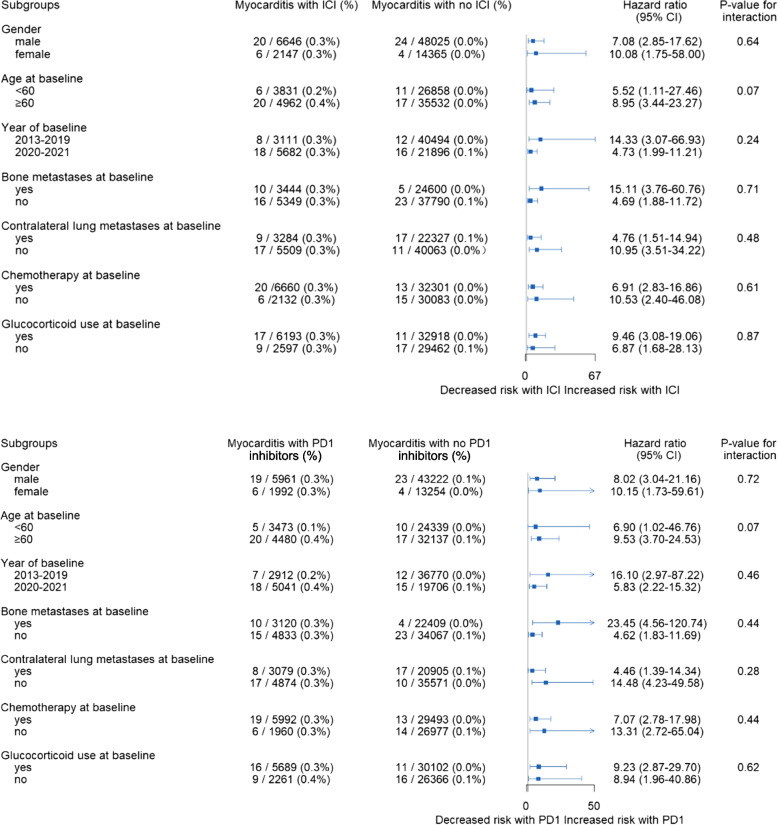
Results: 55,219 patients were included. The median age was 61 years, and 62% were males. At one-year follow-up (median 335 days), there were 26 cases of myocarditis among ICI users and 28 cases among ICI non-users (a cumulative incidence of 4.8 and 0.6 per 1000 person-years respectively). The adjusted hazard ratio (HR) of myocarditis for ICI users was 7.41 (95% confidence interval [CI]: 3.29-16.67). For programmed cell death protein 1 inhibitor users the HR was 8.39 (95% CI: 3.56-19.77). No significant interactions were observed in subgroup analysis. The results remained unchanged in sensitivity analyses.
Conclusions: This study showed that ICI therapy considerably increased the risk of myocarditis, supporting the need for closer monitoring of patients receiving ICI therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


