Maria Stefopoulou, Jonas Johnson, Peter Lindgren, Ganesh Acharya
{"title":"迟发性胎儿生长受限时上腔静脉血流和脑保留的多普勒指数。","authors":"Maria Stefopoulou, Jonas Johnson, Peter Lindgren, Ganesh Acharya","doi":"10.1038/s41598-025-94621-x","DOIUrl":null,"url":null,"abstract":"<p><p>Cerebral hemodynamic adaptation in fetal growth restriction (FGR) is primarily assessed using middle cerebral artery (MCA) Doppler and cerebroplacental (CPR) or umbilicocerebral ratio (UCR). The superior vena cava (SVC) blood flow may provide additional hemodynamic insights. Our objective was to evaluate fetal SVC blood flow velocities, pulsatility index for vein (PIV), volume blood flow (QSVC), and volume blood flow (Q)-based indices of fetal brain sparing in small-for-gestational-age (SGA) and FGR fetuses in the third trimester of pregnancy and compare with appropriately grown (AGA) fetuses. This was a prospective cohort study of 40 non-anomalous, singleton fetuses during 32 + 0 to 36 + 6 gestational weeks. Fetuses with abdominal circumference or estimated fetal weight below the 10th percentile were classified into SGA and FGR groups based on Delphi criteria. Doppler velocimetry of the umbilical artery (UA), umbilical vein (UV), fetal MCA and SVC was performed. UV and SVC diameters were measured, and their volume blood flows, i.e. QUV and QSVC were calculated. Both pulsatility index (PI)-based and Q-based indices of fetal brain sparing were calculated and compared to previously reported reference ranges for AGA fetuses using z-scores. In our study population, z-scores of SVC velocities (except the end-diastolic A-wave velocity) and PIV were significantly lower than the gestational age-specific mean values for AGA fetuses (p-values 0.005 to 0.018). Similarly, z-scores of SVC diameter (p < 0.001), QSVC normalized to fetal weight (QSVCw) (p < 0.001), blood flow volume-based QCPR (p < 0.001) were higher and QUCR (p < 0.001) was lower. However, z-scores of PI-based CPR (p = 0.195), UCR (p = 0.195), and the end-diastolic (A wave) velocity (p = 0.177) were not significantly different compared to AGA fetuses. Subgroup analysis demonstrated that the FGR fetuses (n = 21) had increased SVC diameter (p < 0.001), QSVCw (p < 0.001), QCPR (p < 0.001), UCR (p < 0.001), and decreased CPR (p < 0.001), QUCR (p < 0.001) and SVC PIV (p = 0.030), but no significant change in velocities was observed compared to AGA fetuses (n = 98) of similar gestational age. The SGA fetuses (n = 19) had decreased SVC S velocity (p = 0.013), D velocity (p = 0.005), TAMxV (p = 0.030), PIV (p = 0.005), QUCR (p = 0.014), and increased SVC diameter (p = 0.026), QSVCw (p = 0.034) and QCPR (p = 0.014) in comparison to AGA fetuses. When compared to SGA fetuses, the FGR fetuses had significantly lower QUVw (60.5 ± 19.7 vs. 80.1 ± 20.2 ml/min/kg, p = 0.004), QUCR (0.79 ± 0.45 vs. 1.34 ± 0.52 p < 0.001) and birthweight (2181 ± 577 vs. 2848 ± 330 g, p < 0.001) but higher QSVCw (91.82 ± 39.56 vs. 65.53 ± 17.79 ml/min/kg, p = 0.039) and QCPR (1.63 ± 0.74 vs. 0.90 ± 0.45, p < 0.001). In conclusion, third-trimester fetuses < 10th percentile had significantly increased SVC diameter, resulting in increased QSVCw in SGA and FGR despite reduced or unchanged TAMxV. Significantly altered QCPR and QUCR confirmed circulatory redistribution with increased brain and upper body venous return both in FGR and SGA fetuses. However, as the magnitude of increase in QSVCw and QCPR was significantly larger in FGR compared to SGA fetuses, it could be potentially used as a quantifiable marker to differentiate FGR from SGA. The role of SVC Doppler in refining the diagnosis of late FGR should be further investigated.</p>","PeriodicalId":21811,"journal":{"name":"Scientific Reports","volume":"15 1","pages":"10610"},"PeriodicalIF":3.9000,"publicationDate":"2025-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11950425/pdf/","citationCount":"0","resultStr":"{\"title\":\"Superior vena cava blood flow and Doppler indices of brain sparing in late onset fetal growth restriction.\",\"authors\":\"Maria Stefopoulou, Jonas Johnson, Peter Lindgren, Ganesh Acharya\",\"doi\":\"10.1038/s41598-025-94621-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Cerebral hemodynamic adaptation in fetal growth restriction (FGR) is primarily assessed using middle cerebral artery (MCA) Doppler and cerebroplacental (CPR) or umbilicocerebral ratio (UCR). The superior vena cava (SVC) blood flow may provide additional hemodynamic insights. Our objective was to evaluate fetal SVC blood flow velocities, pulsatility index for vein (PIV), volume blood flow (QSVC), and volume blood flow (Q)-based indices of fetal brain sparing in small-for-gestational-age (SGA) and FGR fetuses in the third trimester of pregnancy and compare with appropriately grown (AGA) fetuses. This was a prospective cohort study of 40 non-anomalous, singleton fetuses during 32 + 0 to 36 + 6 gestational weeks. Fetuses with abdominal circumference or estimated fetal weight below the 10th percentile were classified into SGA and FGR groups based on Delphi criteria. Doppler velocimetry of the umbilical artery (UA), umbilical vein (UV), fetal MCA and SVC was performed. UV and SVC diameters were measured, and their volume blood flows, i.e. QUV and QSVC were calculated. Both pulsatility index (PI)-based and Q-based indices of fetal brain sparing were calculated and compared to previously reported reference ranges for AGA fetuses using z-scores. In our study population, z-scores of SVC velocities (except the end-diastolic A-wave velocity) and PIV were significantly lower than the gestational age-specific mean values for AGA fetuses (p-values 0.005 to 0.018). Similarly, z-scores of SVC diameter (p < 0.001), QSVC normalized to fetal weight (QSVCw) (p < 0.001), blood flow volume-based QCPR (p < 0.001) were higher and QUCR (p < 0.001) was lower. However, z-scores of PI-based CPR (p = 0.195), UCR (p = 0.195), and the end-diastolic (A wave) velocity (p = 0.177) were not significantly different compared to AGA fetuses. Subgroup analysis demonstrated that the FGR fetuses (n = 21) had increased SVC diameter (p < 0.001), QSVCw (p < 0.001), QCPR (p < 0.001), UCR (p < 0.001), and decreased CPR (p < 0.001), QUCR (p < 0.001) and SVC PIV (p = 0.030), but no significant change in velocities was observed compared to AGA fetuses (n = 98) of similar gestational age. The SGA fetuses (n = 19) had decreased SVC S velocity (p = 0.013), D velocity (p = 0.005), TAMxV (p = 0.030), PIV (p = 0.005), QUCR (p = 0.014), and increased SVC diameter (p = 0.026), QSVCw (p = 0.034) and QCPR (p = 0.014) in comparison to AGA fetuses. When compared to SGA fetuses, the FGR fetuses had significantly lower QUVw (60.5 ± 19.7 vs. 80.1 ± 20.2 ml/min/kg, p = 0.004), QUCR (0.79 ± 0.45 vs. 1.34 ± 0.52 p < 0.001) and birthweight (2181 ± 577 vs. 2848 ± 330 g, p < 0.001) but higher QSVCw (91.82 ± 39.56 vs. 65.53 ± 17.79 ml/min/kg, p = 0.039) and QCPR (1.63 ± 0.74 vs. 0.90 ± 0.45, p < 0.001). In conclusion, third-trimester fetuses < 10th percentile had significantly increased SVC diameter, resulting in increased QSVCw in SGA and FGR despite reduced or unchanged TAMxV. Significantly altered QCPR and QUCR confirmed circulatory redistribution with increased brain and upper body venous return both in FGR and SGA fetuses. However, as the magnitude of increase in QSVCw and QCPR was significantly larger in FGR compared to SGA fetuses, it could be potentially used as a quantifiable marker to differentiate FGR from SGA. The role of SVC Doppler in refining the diagnosis of late FGR should be further investigated.</p>\",\"PeriodicalId\":21811,\"journal\":{\"name\":\"Scientific Reports\",\"volume\":\"15 1\",\"pages\":\"10610\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2025-03-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11950425/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scientific Reports\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1038/s41598-025-94621-x\",\"RegionNum\":2,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scientific Reports","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1038/s41598-025-94621-x","RegionNum":2,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Superior vena cava blood flow and Doppler indices of brain sparing in late onset fetal growth restriction.
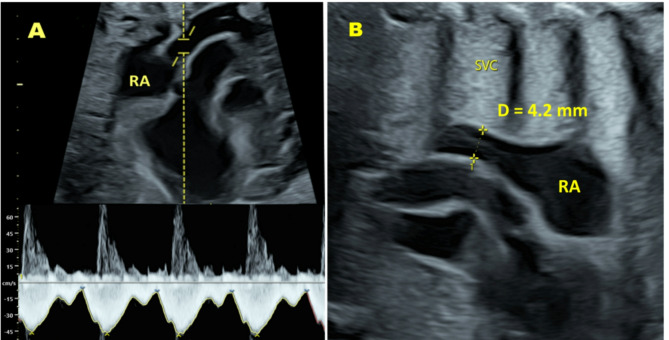
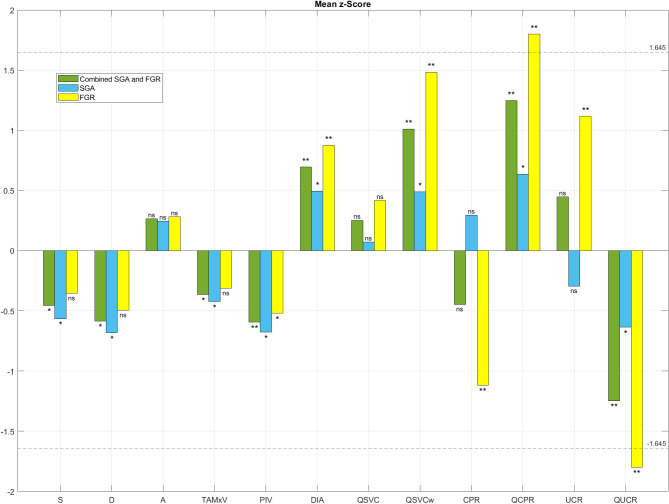
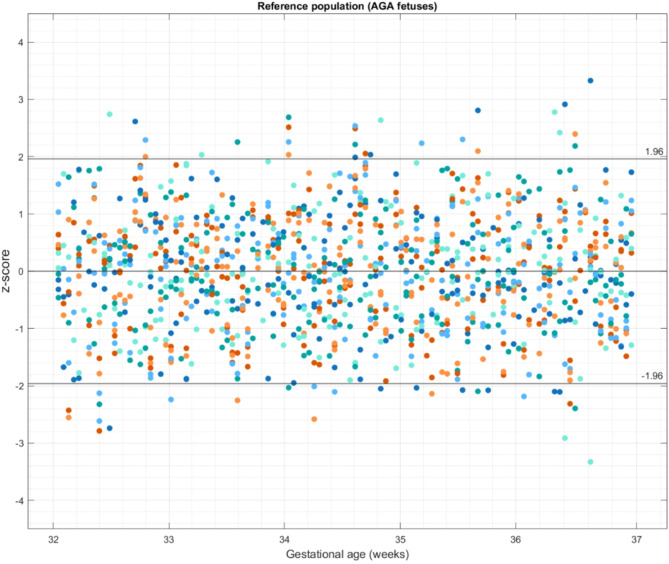
Cerebral hemodynamic adaptation in fetal growth restriction (FGR) is primarily assessed using middle cerebral artery (MCA) Doppler and cerebroplacental (CPR) or umbilicocerebral ratio (UCR). The superior vena cava (SVC) blood flow may provide additional hemodynamic insights. Our objective was to evaluate fetal SVC blood flow velocities, pulsatility index for vein (PIV), volume blood flow (QSVC), and volume blood flow (Q)-based indices of fetal brain sparing in small-for-gestational-age (SGA) and FGR fetuses in the third trimester of pregnancy and compare with appropriately grown (AGA) fetuses. This was a prospective cohort study of 40 non-anomalous, singleton fetuses during 32 + 0 to 36 + 6 gestational weeks. Fetuses with abdominal circumference or estimated fetal weight below the 10th percentile were classified into SGA and FGR groups based on Delphi criteria. Doppler velocimetry of the umbilical artery (UA), umbilical vein (UV), fetal MCA and SVC was performed. UV and SVC diameters were measured, and their volume blood flows, i.e. QUV and QSVC were calculated. Both pulsatility index (PI)-based and Q-based indices of fetal brain sparing were calculated and compared to previously reported reference ranges for AGA fetuses using z-scores. In our study population, z-scores of SVC velocities (except the end-diastolic A-wave velocity) and PIV were significantly lower than the gestational age-specific mean values for AGA fetuses (p-values 0.005 to 0.018). Similarly, z-scores of SVC diameter (p < 0.001), QSVC normalized to fetal weight (QSVCw) (p < 0.001), blood flow volume-based QCPR (p < 0.001) were higher and QUCR (p < 0.001) was lower. However, z-scores of PI-based CPR (p = 0.195), UCR (p = 0.195), and the end-diastolic (A wave) velocity (p = 0.177) were not significantly different compared to AGA fetuses. Subgroup analysis demonstrated that the FGR fetuses (n = 21) had increased SVC diameter (p < 0.001), QSVCw (p < 0.001), QCPR (p < 0.001), UCR (p < 0.001), and decreased CPR (p < 0.001), QUCR (p < 0.001) and SVC PIV (p = 0.030), but no significant change in velocities was observed compared to AGA fetuses (n = 98) of similar gestational age. The SGA fetuses (n = 19) had decreased SVC S velocity (p = 0.013), D velocity (p = 0.005), TAMxV (p = 0.030), PIV (p = 0.005), QUCR (p = 0.014), and increased SVC diameter (p = 0.026), QSVCw (p = 0.034) and QCPR (p = 0.014) in comparison to AGA fetuses. When compared to SGA fetuses, the FGR fetuses had significantly lower QUVw (60.5 ± 19.7 vs. 80.1 ± 20.2 ml/min/kg, p = 0.004), QUCR (0.79 ± 0.45 vs. 1.34 ± 0.52 p < 0.001) and birthweight (2181 ± 577 vs. 2848 ± 330 g, p < 0.001) but higher QSVCw (91.82 ± 39.56 vs. 65.53 ± 17.79 ml/min/kg, p = 0.039) and QCPR (1.63 ± 0.74 vs. 0.90 ± 0.45, p < 0.001). In conclusion, third-trimester fetuses < 10th percentile had significantly increased SVC diameter, resulting in increased QSVCw in SGA and FGR despite reduced or unchanged TAMxV. Significantly altered QCPR and QUCR confirmed circulatory redistribution with increased brain and upper body venous return both in FGR and SGA fetuses. However, as the magnitude of increase in QSVCw and QCPR was significantly larger in FGR compared to SGA fetuses, it could be potentially used as a quantifiable marker to differentiate FGR from SGA. The role of SVC Doppler in refining the diagnosis of late FGR should be further investigated.
期刊介绍:
We publish original research from all areas of the natural sciences, psychology, medicine and engineering. You can learn more about what we publish by browsing our specific scientific subject areas below or explore Scientific Reports by browsing all articles and collections.
Scientific Reports has a 2-year impact factor: 4.380 (2021), and is the 6th most-cited journal in the world, with more than 540,000 citations in 2020 (Clarivate Analytics, 2021).
•Engineering
Engineering covers all aspects of engineering, technology, and applied science. It plays a crucial role in the development of technologies to address some of the world''s biggest challenges, helping to save lives and improve the way we live.
•Physical sciences
Physical sciences are those academic disciplines that aim to uncover the underlying laws of nature — often written in the language of mathematics. It is a collective term for areas of study including astronomy, chemistry, materials science and physics.
•Earth and environmental sciences
Earth and environmental sciences cover all aspects of Earth and planetary science and broadly encompass solid Earth processes, surface and atmospheric dynamics, Earth system history, climate and climate change, marine and freshwater systems, and ecology. It also considers the interactions between humans and these systems.
•Biological sciences
Biological sciences encompass all the divisions of natural sciences examining various aspects of vital processes. The concept includes anatomy, physiology, cell biology, biochemistry and biophysics, and covers all organisms from microorganisms, animals to plants.
•Health sciences
The health sciences study health, disease and healthcare. This field of study aims to develop knowledge, interventions and technology for use in healthcare to improve the treatment of patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


