Joanna Furnival-Adams, Amelia Houana, Patricia Nicolas, Julia Montaña, Samuel Martinho, Aina Casellas, Hansel Mundaca, Jenisse Mbanze, Arlindo Soares, Saimado Imputiua, Paula Ruiz-Castillo, Marta Ribes, Almudena Sanz, Mussa Mamudo Salé, Antonio Macucha, Eldo Elobolobo, Vegovito Vegove, Victor Mutepa, Humberto Munguambe, Aida Xerinda, Felisbela Materula, Regina Rabinovich, Francisco Saute, Carlos Chaccour
{"title":"在莫桑比克莫皮亚设计用于治疗头虱疟疾的伊维菌素大规模给药的附带效益:一项聚类随机对照试验。","authors":"Joanna Furnival-Adams, Amelia Houana, Patricia Nicolas, Julia Montaña, Samuel Martinho, Aina Casellas, Hansel Mundaca, Jenisse Mbanze, Arlindo Soares, Saimado Imputiua, Paula Ruiz-Castillo, Marta Ribes, Almudena Sanz, Mussa Mamudo Salé, Antonio Macucha, Eldo Elobolobo, Vegovito Vegove, Victor Mutepa, Humberto Munguambe, Aida Xerinda, Felisbela Materula, Regina Rabinovich, Francisco Saute, Carlos Chaccour","doi":"10.1186/s40249-025-01290-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Headlice are prevalent worldwide, with a higher burden in rural, lower-middle income settings. They can cause intense itchiness, discomfort, and secondary bacterial infections with potentially serious consequences. Ivermectin is efficacious against headlice, and is also being evaluated as a malaria vector control tool. In this study, we explored risk factors for headlice, and assessed the efficacy of ivermectin mass drug administration (MDA) designed for malaria against headlice.</p><p><strong>Methods: </strong>We conducted an open-label, assessor-blind, cluster-randomized controlled trial in Mopeia, Mozambique. A single dose of ivermectin was given monthly to eligible humans or humans and livestock (humans: 400 μg/kg, livestock: 1% injectable 200 μg/kg) in 3 consecutive months during the rainy season. The control group received albendazole (humans only). Thirty-nine clusters (13 per arm) were randomly selected for the nested assessment of headlice prevalence. 1341 treated participants were followed up at least once, 1, 2 and 3 months and 382 untreated (ineligible) participants at 3 and 6 months after the first MDA round. Headlice diagnosis was determined by scalp examination. Logistic regression was used to identify risk factors for headlice at baseline, and to estimate the treatment effect at each time point.</p><p><strong>Results: </strong>A total of 1309 participants were included in the main analysis assessing ivermectin MDA efficacy, and 1332 in the risk factor analysis. The baseline headlice prevalence was 11%. Risk factors included living with a household member with head itch [adjusted odds ratio (aOR) = 48.63, 95% confidence interval (CI): 28.7-82.3, P-value < 0.0001], being female (aOR = 2.25, 95% CI: 1.33-3.80, P-value < 0.01), and using surface water as the main water (aOR = 2.37, 95% CI: 1.12-5.33, P-value = 0.04). The treated population receiving ivermectin had significantly lower odds of having headlice at 3 months compared to those receiving albendazole (aOR = 0.19, 95% CI: 0.04-0.91, P-value = 0.04). There was no indirect effect on headlice among children ineligible for treatment.</p><p><strong>Conclusions: </strong>In a highly endemic setting, mass drug administration with ivermectin significantly reduces headlice infestation prevalence among those who receive the drug for three sequential months. The lack of effect among untreated, ineligible children implies that additional interventions would be needed to interrupt local transmission.</p><p><strong>Trial registration: </strong>This study is registered with ClinicalTrials.gov (NCT04966702).</p>","PeriodicalId":48820,"journal":{"name":"Infectious Diseases of Poverty","volume":"14 1","pages":"25"},"PeriodicalIF":5.5000,"publicationDate":"2025-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11948683/pdf/","citationCount":"0","resultStr":"{\"title\":\"Collateral benefits of ivermectin mass drug administration designed for malaria against headlice in Mopeia, Mozambique: a cluster randomised controlled trial.\",\"authors\":\"Joanna Furnival-Adams, Amelia Houana, Patricia Nicolas, Julia Montaña, Samuel Martinho, Aina Casellas, Hansel Mundaca, Jenisse Mbanze, Arlindo Soares, Saimado Imputiua, Paula Ruiz-Castillo, Marta Ribes, Almudena Sanz, Mussa Mamudo Salé, Antonio Macucha, Eldo Elobolobo, Vegovito Vegove, Victor Mutepa, Humberto Munguambe, Aida Xerinda, Felisbela Materula, Regina Rabinovich, Francisco Saute, Carlos Chaccour\",\"doi\":\"10.1186/s40249-025-01290-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Headlice are prevalent worldwide, with a higher burden in rural, lower-middle income settings. They can cause intense itchiness, discomfort, and secondary bacterial infections with potentially serious consequences. Ivermectin is efficacious against headlice, and is also being evaluated as a malaria vector control tool. In this study, we explored risk factors for headlice, and assessed the efficacy of ivermectin mass drug administration (MDA) designed for malaria against headlice.</p><p><strong>Methods: </strong>We conducted an open-label, assessor-blind, cluster-randomized controlled trial in Mopeia, Mozambique. A single dose of ivermectin was given monthly to eligible humans or humans and livestock (humans: 400 μg/kg, livestock: 1% injectable 200 μg/kg) in 3 consecutive months during the rainy season. The control group received albendazole (humans only). Thirty-nine clusters (13 per arm) were randomly selected for the nested assessment of headlice prevalence. 1341 treated participants were followed up at least once, 1, 2 and 3 months and 382 untreated (ineligible) participants at 3 and 6 months after the first MDA round. Headlice diagnosis was determined by scalp examination. Logistic regression was used to identify risk factors for headlice at baseline, and to estimate the treatment effect at each time point.</p><p><strong>Results: </strong>A total of 1309 participants were included in the main analysis assessing ivermectin MDA efficacy, and 1332 in the risk factor analysis. The baseline headlice prevalence was 11%. Risk factors included living with a household member with head itch [adjusted odds ratio (aOR) = 48.63, 95% confidence interval (CI): 28.7-82.3, P-value < 0.0001], being female (aOR = 2.25, 95% CI: 1.33-3.80, P-value < 0.01), and using surface water as the main water (aOR = 2.37, 95% CI: 1.12-5.33, P-value = 0.04). The treated population receiving ivermectin had significantly lower odds of having headlice at 3 months compared to those receiving albendazole (aOR = 0.19, 95% CI: 0.04-0.91, P-value = 0.04). There was no indirect effect on headlice among children ineligible for treatment.</p><p><strong>Conclusions: </strong>In a highly endemic setting, mass drug administration with ivermectin significantly reduces headlice infestation prevalence among those who receive the drug for three sequential months. The lack of effect among untreated, ineligible children implies that additional interventions would be needed to interrupt local transmission.</p><p><strong>Trial registration: </strong>This study is registered with ClinicalTrials.gov (NCT04966702).</p>\",\"PeriodicalId\":48820,\"journal\":{\"name\":\"Infectious Diseases of Poverty\",\"volume\":\"14 1\",\"pages\":\"25\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2025-03-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11948683/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Diseases of Poverty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40249-025-01290-z\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases of Poverty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40249-025-01290-z","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Collateral benefits of ivermectin mass drug administration designed for malaria against headlice in Mopeia, Mozambique: a cluster randomised controlled trial.
Background: Headlice are prevalent worldwide, with a higher burden in rural, lower-middle income settings. They can cause intense itchiness, discomfort, and secondary bacterial infections with potentially serious consequences. Ivermectin is efficacious against headlice, and is also being evaluated as a malaria vector control tool. In this study, we explored risk factors for headlice, and assessed the efficacy of ivermectin mass drug administration (MDA) designed for malaria against headlice.
Methods: We conducted an open-label, assessor-blind, cluster-randomized controlled trial in Mopeia, Mozambique. A single dose of ivermectin was given monthly to eligible humans or humans and livestock (humans: 400 μg/kg, livestock: 1% injectable 200 μg/kg) in 3 consecutive months during the rainy season. The control group received albendazole (humans only). Thirty-nine clusters (13 per arm) were randomly selected for the nested assessment of headlice prevalence. 1341 treated participants were followed up at least once, 1, 2 and 3 months and 382 untreated (ineligible) participants at 3 and 6 months after the first MDA round. Headlice diagnosis was determined by scalp examination. Logistic regression was used to identify risk factors for headlice at baseline, and to estimate the treatment effect at each time point.
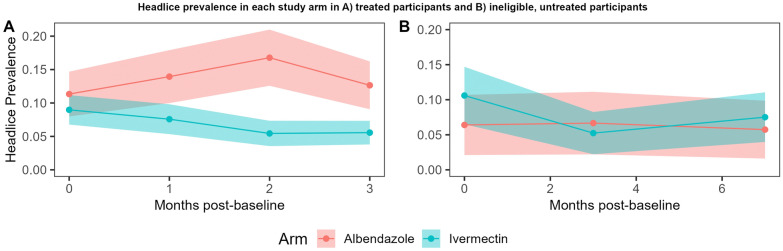
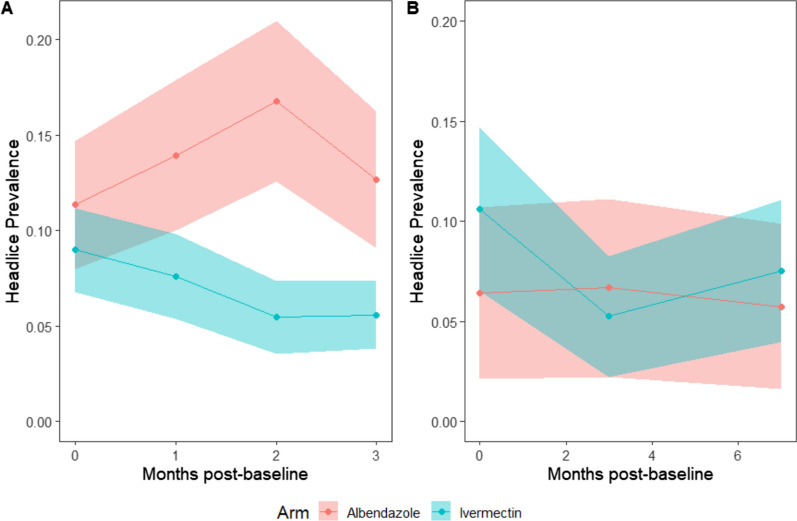
Results: A total of 1309 participants were included in the main analysis assessing ivermectin MDA efficacy, and 1332 in the risk factor analysis. The baseline headlice prevalence was 11%. Risk factors included living with a household member with head itch [adjusted odds ratio (aOR) = 48.63, 95% confidence interval (CI): 28.7-82.3, P-value < 0.0001], being female (aOR = 2.25, 95% CI: 1.33-3.80, P-value < 0.01), and using surface water as the main water (aOR = 2.37, 95% CI: 1.12-5.33, P-value = 0.04). The treated population receiving ivermectin had significantly lower odds of having headlice at 3 months compared to those receiving albendazole (aOR = 0.19, 95% CI: 0.04-0.91, P-value = 0.04). There was no indirect effect on headlice among children ineligible for treatment.
Conclusions: In a highly endemic setting, mass drug administration with ivermectin significantly reduces headlice infestation prevalence among those who receive the drug for three sequential months. The lack of effect among untreated, ineligible children implies that additional interventions would be needed to interrupt local transmission.
Trial registration: This study is registered with ClinicalTrials.gov (NCT04966702).
期刊介绍:
Infectious Diseases of Poverty is an open access, peer-reviewed journal that focuses on addressing essential public health questions related to infectious diseases of poverty. The journal covers a wide range of topics including the biology of pathogens and vectors, diagnosis and detection, treatment and case management, epidemiology and modeling, zoonotic hosts and animal reservoirs, control strategies and implementation, new technologies and application. It also considers the transdisciplinary or multisectoral effects on health systems, ecohealth, environmental management, and innovative technology. The journal aims to identify and assess research and information gaps that hinder progress towards new interventions for public health problems in the developing world. Additionally, it provides a platform for discussing these issues to advance research and evidence building for improved public health interventions in poor settings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


