{"title":"三级医院妇科机器人手术的安全实施:149例回顾性分析及文献复习。","authors":"Takuma Yoshimura, Hiroshi Nishio, Kensuke Sakai, Yuya Nogami, Shigenori Hayashi, Wataru Yamagami","doi":"10.4103/gmit.gmit_144_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The initial learning curve is a barrier to introducing robotic surgery. Evidence regarding appropriate simulation programs that allow for a smooth introduction of gynecological robotic surgery remains limited.</p><p><strong>Materials and methods: </strong>We retrospectively analyzed 149 patients who underwent robotic surgery for gynecologic diseases. Before their first procedure, the surgeons completed a robotic surgery training program. Assistant surgeons also completed simulation programs, including setup procedures and manipulation of the robotic arm.</p><p><strong>Results: </strong>The mean (± standard deviation) operative, setup, and console times were 170 ± 54 min, 22 ± 8 min, and 126 ± 51 min, respectively. No patient required blood transfusion or conversion to laparoscopy or laparotomy. Patients undergoing surgery by the same surgeon were divided into three groups (first-third, middle-third, and last-third of patients undergoing surgery) to assess chronological changes. No statistically significant differences were found between the operative and console times among these groups. The setup times for the middle and last third of patients were 20 ± 7 min and 18 ± 7 min, respectively, which were statistically significantly shorter than those for the first third of patients. No significant differences in the operative and console times done by five physicians who completed programs were observed between the first 75 and the latter 74 procedures; however, the setup times of the latter 74 procedures were significantly shorter than those of the first 74 procedures (25 ± 9 min vs. 19 ± 6 min; <i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>The setup time was influenced by clinical experience. An appropriate simulation program allowed a safe implementation of robotic surgery.</p>","PeriodicalId":45272,"journal":{"name":"Gynecology and Minimally Invasive Therapy-GMIT","volume":"14 1","pages":"33-39"},"PeriodicalIF":1.7000,"publicationDate":"2024-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11936396/pdf/","citationCount":"0","resultStr":"{\"title\":\"Safe Implementation of Robotic Surgery for Gynecologic Diseases at a Tertiary Center: Retrospective Analysis of 149 Cases and Review of the Literature.\",\"authors\":\"Takuma Yoshimura, Hiroshi Nishio, Kensuke Sakai, Yuya Nogami, Shigenori Hayashi, Wataru Yamagami\",\"doi\":\"10.4103/gmit.gmit_144_23\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The initial learning curve is a barrier to introducing robotic surgery. Evidence regarding appropriate simulation programs that allow for a smooth introduction of gynecological robotic surgery remains limited.</p><p><strong>Materials and methods: </strong>We retrospectively analyzed 149 patients who underwent robotic surgery for gynecologic diseases. Before their first procedure, the surgeons completed a robotic surgery training program. Assistant surgeons also completed simulation programs, including setup procedures and manipulation of the robotic arm.</p><p><strong>Results: </strong>The mean (± standard deviation) operative, setup, and console times were 170 ± 54 min, 22 ± 8 min, and 126 ± 51 min, respectively. No patient required blood transfusion or conversion to laparoscopy or laparotomy. Patients undergoing surgery by the same surgeon were divided into three groups (first-third, middle-third, and last-third of patients undergoing surgery) to assess chronological changes. No statistically significant differences were found between the operative and console times among these groups. The setup times for the middle and last third of patients were 20 ± 7 min and 18 ± 7 min, respectively, which were statistically significantly shorter than those for the first third of patients. No significant differences in the operative and console times done by five physicians who completed programs were observed between the first 75 and the latter 74 procedures; however, the setup times of the latter 74 procedures were significantly shorter than those of the first 74 procedures (25 ± 9 min vs. 19 ± 6 min; <i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>The setup time was influenced by clinical experience. An appropriate simulation program allowed a safe implementation of robotic surgery.</p>\",\"PeriodicalId\":45272,\"journal\":{\"name\":\"Gynecology and Minimally Invasive Therapy-GMIT\",\"volume\":\"14 1\",\"pages\":\"33-39\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-12-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11936396/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gynecology and Minimally Invasive Therapy-GMIT\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/gmit.gmit_144_23\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecology and Minimally Invasive Therapy-GMIT","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/gmit.gmit_144_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Safe Implementation of Robotic Surgery for Gynecologic Diseases at a Tertiary Center: Retrospective Analysis of 149 Cases and Review of the Literature.
Objectives: The initial learning curve is a barrier to introducing robotic surgery. Evidence regarding appropriate simulation programs that allow for a smooth introduction of gynecological robotic surgery remains limited.
Materials and methods: We retrospectively analyzed 149 patients who underwent robotic surgery for gynecologic diseases. Before their first procedure, the surgeons completed a robotic surgery training program. Assistant surgeons also completed simulation programs, including setup procedures and manipulation of the robotic arm.
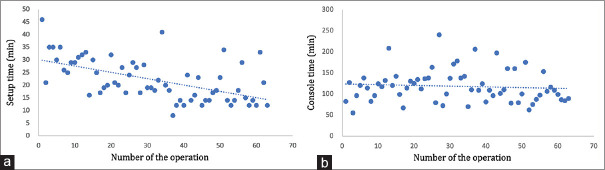
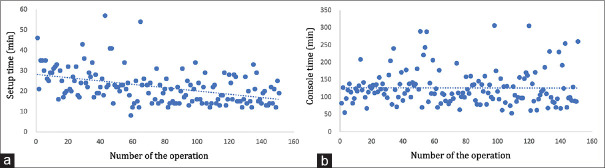
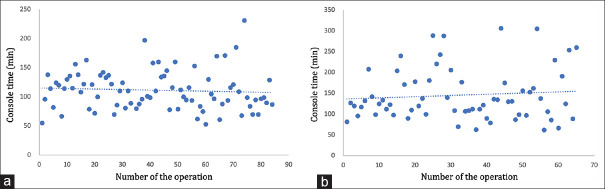
Results: The mean (± standard deviation) operative, setup, and console times were 170 ± 54 min, 22 ± 8 min, and 126 ± 51 min, respectively. No patient required blood transfusion or conversion to laparoscopy or laparotomy. Patients undergoing surgery by the same surgeon were divided into three groups (first-third, middle-third, and last-third of patients undergoing surgery) to assess chronological changes. No statistically significant differences were found between the operative and console times among these groups. The setup times for the middle and last third of patients were 20 ± 7 min and 18 ± 7 min, respectively, which were statistically significantly shorter than those for the first third of patients. No significant differences in the operative and console times done by five physicians who completed programs were observed between the first 75 and the latter 74 procedures; however, the setup times of the latter 74 procedures were significantly shorter than those of the first 74 procedures (25 ± 9 min vs. 19 ± 6 min; P < 0.001).
Conclusion: The setup time was influenced by clinical experience. An appropriate simulation program allowed a safe implementation of robotic surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


