{"title":"慢性肾病患者既往房颤与血液透析起始时新发房颤的预后差异:一项回顾性单中心队列研究","authors":"Tomohisa Tsuyuki, Mineaki Kitamura, Haruka Fukuda, Takuma Ishii, Kenta Torigoe, Hiroshi Yamashita, Takahiro Takazono, Noriho Sakamoto, Hiroshi Mukae, Tomoya Nishino","doi":"10.1371/journal.pone.0320336","DOIUrl":null,"url":null,"abstract":"<p><p>Atrial fibrillation (AF) can develop in patients with chronic kidney disease. However, the impact of new-onset AF in patients who are initiated on hemodialysis remains unclear. We categorized 254 patients who were started on hemodialysis into three groups: those with pre-existing AF, those with new-onset AF, and those without AF. Statistical analyses were performed to evaluate the associations between patient characteristics and survival outcomes. AF was observed in 42 patients (16.5%), of whom 19 (7.5%) had pre-existing AF and 23 (9.1%) developed new-onset AF at the initiation of hemodialysis. Multivariate logistic regression models showed that only low serum albumin levels were associated with AF (P = 0.04). Age- and other factors-adjusted multivariable Cox regression models indicated that AF, particularly pre-existing AF, was an independent risk factor for death after dialysis initiation (hazard ratio [HR]: 2.28, 95% confidence interval [CI]: 1.39-3.74, P = 0.001; HR: 3.05, 95% CI: 1.64-5.66, P = 0.004, respectively). However, new-onset AF was not significantly associated with mortality (HR: 1.43, 95% CI: 0.74-2.78, P = 0.28). These findings suggest that pre-existing AF before hemodialysis initiation has a crucial impact on patient prognosis.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 3","pages":"e0320336"},"PeriodicalIF":2.6000,"publicationDate":"2025-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11936237/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic differences between pre-existing atrial fibrillation in chronic kidney disease and new-onset atrial fibrillation at hemodialysis initiation: a retrospective single-center cohort study.\",\"authors\":\"Tomohisa Tsuyuki, Mineaki Kitamura, Haruka Fukuda, Takuma Ishii, Kenta Torigoe, Hiroshi Yamashita, Takahiro Takazono, Noriho Sakamoto, Hiroshi Mukae, Tomoya Nishino\",\"doi\":\"10.1371/journal.pone.0320336\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Atrial fibrillation (AF) can develop in patients with chronic kidney disease. However, the impact of new-onset AF in patients who are initiated on hemodialysis remains unclear. We categorized 254 patients who were started on hemodialysis into three groups: those with pre-existing AF, those with new-onset AF, and those without AF. Statistical analyses were performed to evaluate the associations between patient characteristics and survival outcomes. AF was observed in 42 patients (16.5%), of whom 19 (7.5%) had pre-existing AF and 23 (9.1%) developed new-onset AF at the initiation of hemodialysis. Multivariate logistic regression models showed that only low serum albumin levels were associated with AF (P = 0.04). Age- and other factors-adjusted multivariable Cox regression models indicated that AF, particularly pre-existing AF, was an independent risk factor for death after dialysis initiation (hazard ratio [HR]: 2.28, 95% confidence interval [CI]: 1.39-3.74, P = 0.001; HR: 3.05, 95% CI: 1.64-5.66, P = 0.004, respectively). However, new-onset AF was not significantly associated with mortality (HR: 1.43, 95% CI: 0.74-2.78, P = 0.28). These findings suggest that pre-existing AF before hemodialysis initiation has a crucial impact on patient prognosis.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 3\",\"pages\":\"e0320336\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-03-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11936237/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0320336\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0320336","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
摘要
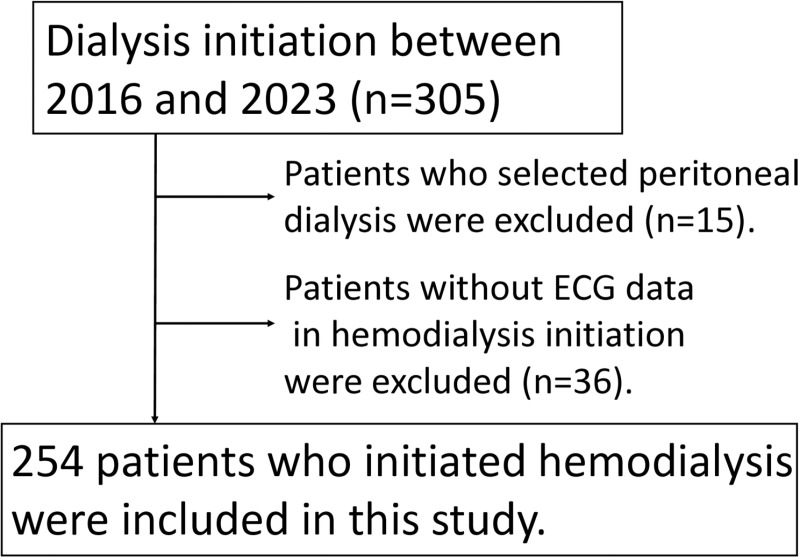
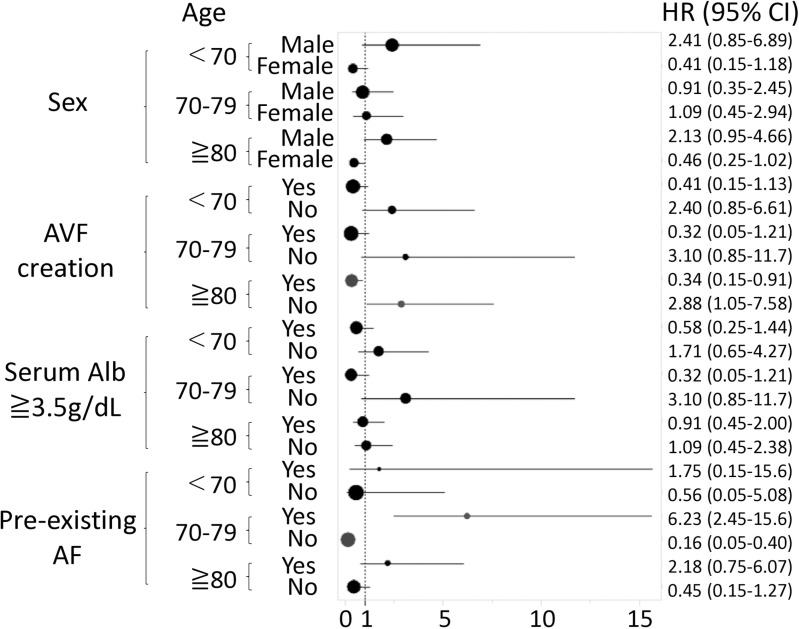
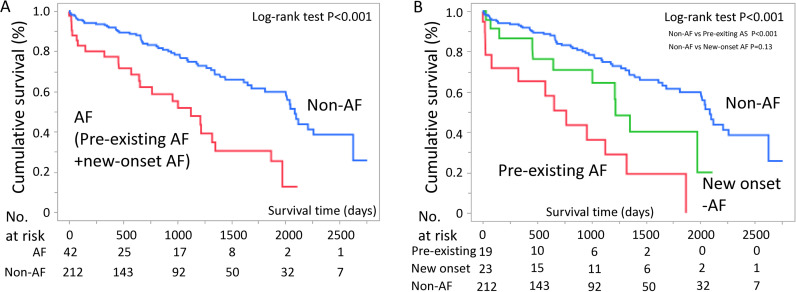
慢性肾脏疾病患者可发生心房颤动(AF)。然而,新发房颤对血液透析患者的影响尚不清楚。我们将254名开始进行血液透析的患者分为三组:既往房颤患者、新发房颤患者和无房颤患者。进行统计学分析以评估患者特征与生存结果之间的关系。42例(16.5%)患者出现房颤,其中19例(7.5%)已存在房颤,23例(9.1%)在血液透析开始时出现新发房颤。多因素logistic回归模型显示,只有低血清白蛋白水平与房颤相关(P = 0.04)。经年龄和其他因素调整的多变量Cox回归模型显示,房颤,特别是既往房颤,是透析开始后死亡的独立危险因素(风险比[HR]: 2.28, 95%可信区间[CI]: 1.39-3.74, P = 0.001;HR: 3.05, 95% CI: 1.64-5.66, P = 0.004)。然而,新发房颤与死亡率无显著相关性(HR: 1.43, 95% CI: 0.74-2.78, P = 0.28)。这些发现表明,血液透析开始前存在的房颤对患者预后有重要影响。
Prognostic differences between pre-existing atrial fibrillation in chronic kidney disease and new-onset atrial fibrillation at hemodialysis initiation: a retrospective single-center cohort study.
Atrial fibrillation (AF) can develop in patients with chronic kidney disease. However, the impact of new-onset AF in patients who are initiated on hemodialysis remains unclear. We categorized 254 patients who were started on hemodialysis into three groups: those with pre-existing AF, those with new-onset AF, and those without AF. Statistical analyses were performed to evaluate the associations between patient characteristics and survival outcomes. AF was observed in 42 patients (16.5%), of whom 19 (7.5%) had pre-existing AF and 23 (9.1%) developed new-onset AF at the initiation of hemodialysis. Multivariate logistic regression models showed that only low serum albumin levels were associated with AF (P = 0.04). Age- and other factors-adjusted multivariable Cox regression models indicated that AF, particularly pre-existing AF, was an independent risk factor for death after dialysis initiation (hazard ratio [HR]: 2.28, 95% confidence interval [CI]: 1.39-3.74, P = 0.001; HR: 3.05, 95% CI: 1.64-5.66, P = 0.004, respectively). However, new-onset AF was not significantly associated with mortality (HR: 1.43, 95% CI: 0.74-2.78, P = 0.28). These findings suggest that pre-existing AF before hemodialysis initiation has a crucial impact on patient prognosis.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


