{"title":"39岁女性原发性腹膜透明细胞癌伴非特异性胃肠道症状1例","authors":"Ramya Vasireddy, Thilini Delungahawatta, Greeshma Gaddipati, Jeffrey Iding, Bryan Szeto, Christopher J Haas","doi":"10.1159/000544883","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Primary peritoneal clear cell carcinoma (PPCCC) is a rare abdominal tumor, affecting 7 out of every million people. Its vague presenting signs and symptoms often lead to delayed diagnosis and poor prognosis. We present a case involving a young woman with anemia and abdominal discomfort who on further investigation had a 26-cm abdominal tumor identified to be PPCCC. Multimodal therapy with tumor debulking and chemotherapy was pursued. Given the aggressive nature of PPCCC, any clinical suspicion of peritoneal carcinoma should prompt thorough diagnostic evaluation.</p><p><strong>Case presentation: </strong>A 39-year-old woman with menorrhagia and peptic ulcer disease presented with abdominal discomfort of 2 days duration. She initially had headaches managed with ibuprofen. Following this, she had generalized abdominal pain with bloating that worsened with food and had no relief with use of stool softeners. She had associated dizziness with palpitations, chest pressure, and exertional dyspnea. In the emergency department, the patient was mildly tachycardic but otherwise stable. On exam, she had a distended abdomen with generalized tenderness and normoactive bowel sounds. Labs showed normocytic anemia with a hemoglobin of 5.2 mg/dL. Electrocardiogram and abdominal and chest X-rays were normal. A non-contrast computed tomography of the abdomen and pelvis showed a fibroid uterus and posterior displacement of multiple bowel loops by a large septate cystic mass (13.5 × 26.0 × 26.7 cm) occupying the entire abdominal cavity. Elevated CA 125 and CA 19-9 were also noted. She underwent exploratory laparotomy with mass resection, partial omentectomy, left colectomy (given extension into transverse colon), appendectomy, and total abdominal hysterectomy with bilateral salpingectomy. Biopsy and immunohistochemical staining (positive for PAX-8, ER, P53, P16, Napsin A and negative for PR and WT-1) confirmed mass as stage IIIB PPCCC. There was no evidence of malignancy in other tissue samples. The patient was discharged with a plan for outpatient chemotherapy and genetic counseling.</p><p><strong>Conclusion: </strong>Given the rarity of PPCCC, our case highlights how increased clinical vigilance and prompt multidisciplinary efforts are essential for an accurate diagnosis, especially in younger patients to not delay management. Currently, there are no established management guidelines; however, initial treatment with surgical debulking followed by chemotherapy is often practiced.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"198-203"},"PeriodicalIF":0.6000,"publicationDate":"2025-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11936432/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary Peritoneal Clear Cell Carcinoma Presenting with Nonspecific Gastrointestinal Symptoms in a 39-Year-Old Woman: A Case Report.\",\"authors\":\"Ramya Vasireddy, Thilini Delungahawatta, Greeshma Gaddipati, Jeffrey Iding, Bryan Szeto, Christopher J Haas\",\"doi\":\"10.1159/000544883\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Primary peritoneal clear cell carcinoma (PPCCC) is a rare abdominal tumor, affecting 7 out of every million people. Its vague presenting signs and symptoms often lead to delayed diagnosis and poor prognosis. We present a case involving a young woman with anemia and abdominal discomfort who on further investigation had a 26-cm abdominal tumor identified to be PPCCC. Multimodal therapy with tumor debulking and chemotherapy was pursued. Given the aggressive nature of PPCCC, any clinical suspicion of peritoneal carcinoma should prompt thorough diagnostic evaluation.</p><p><strong>Case presentation: </strong>A 39-year-old woman with menorrhagia and peptic ulcer disease presented with abdominal discomfort of 2 days duration. She initially had headaches managed with ibuprofen. Following this, she had generalized abdominal pain with bloating that worsened with food and had no relief with use of stool softeners. She had associated dizziness with palpitations, chest pressure, and exertional dyspnea. In the emergency department, the patient was mildly tachycardic but otherwise stable. On exam, she had a distended abdomen with generalized tenderness and normoactive bowel sounds. Labs showed normocytic anemia with a hemoglobin of 5.2 mg/dL. Electrocardiogram and abdominal and chest X-rays were normal. A non-contrast computed tomography of the abdomen and pelvis showed a fibroid uterus and posterior displacement of multiple bowel loops by a large septate cystic mass (13.5 × 26.0 × 26.7 cm) occupying the entire abdominal cavity. Elevated CA 125 and CA 19-9 were also noted. She underwent exploratory laparotomy with mass resection, partial omentectomy, left colectomy (given extension into transverse colon), appendectomy, and total abdominal hysterectomy with bilateral salpingectomy. Biopsy and immunohistochemical staining (positive for PAX-8, ER, P53, P16, Napsin A and negative for PR and WT-1) confirmed mass as stage IIIB PPCCC. There was no evidence of malignancy in other tissue samples. The patient was discharged with a plan for outpatient chemotherapy and genetic counseling.</p><p><strong>Conclusion: </strong>Given the rarity of PPCCC, our case highlights how increased clinical vigilance and prompt multidisciplinary efforts are essential for an accurate diagnosis, especially in younger patients to not delay management. Currently, there are no established management guidelines; however, initial treatment with surgical debulking followed by chemotherapy is often practiced.</p>\",\"PeriodicalId\":9614,\"journal\":{\"name\":\"Case Reports in Gastroenterology\",\"volume\":\"19 1\",\"pages\":\"198-203\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2025-03-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11936432/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000544883\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000544883","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Primary Peritoneal Clear Cell Carcinoma Presenting with Nonspecific Gastrointestinal Symptoms in a 39-Year-Old Woman: A Case Report.
Introduction: Primary peritoneal clear cell carcinoma (PPCCC) is a rare abdominal tumor, affecting 7 out of every million people. Its vague presenting signs and symptoms often lead to delayed diagnosis and poor prognosis. We present a case involving a young woman with anemia and abdominal discomfort who on further investigation had a 26-cm abdominal tumor identified to be PPCCC. Multimodal therapy with tumor debulking and chemotherapy was pursued. Given the aggressive nature of PPCCC, any clinical suspicion of peritoneal carcinoma should prompt thorough diagnostic evaluation.
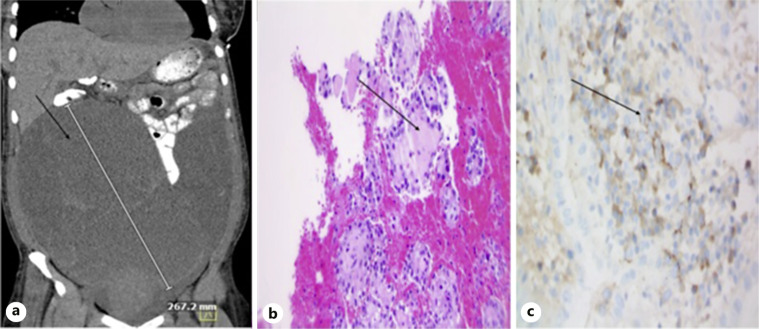
Case presentation: A 39-year-old woman with menorrhagia and peptic ulcer disease presented with abdominal discomfort of 2 days duration. She initially had headaches managed with ibuprofen. Following this, she had generalized abdominal pain with bloating that worsened with food and had no relief with use of stool softeners. She had associated dizziness with palpitations, chest pressure, and exertional dyspnea. In the emergency department, the patient was mildly tachycardic but otherwise stable. On exam, she had a distended abdomen with generalized tenderness and normoactive bowel sounds. Labs showed normocytic anemia with a hemoglobin of 5.2 mg/dL. Electrocardiogram and abdominal and chest X-rays were normal. A non-contrast computed tomography of the abdomen and pelvis showed a fibroid uterus and posterior displacement of multiple bowel loops by a large septate cystic mass (13.5 × 26.0 × 26.7 cm) occupying the entire abdominal cavity. Elevated CA 125 and CA 19-9 were also noted. She underwent exploratory laparotomy with mass resection, partial omentectomy, left colectomy (given extension into transverse colon), appendectomy, and total abdominal hysterectomy with bilateral salpingectomy. Biopsy and immunohistochemical staining (positive for PAX-8, ER, P53, P16, Napsin A and negative for PR and WT-1) confirmed mass as stage IIIB PPCCC. There was no evidence of malignancy in other tissue samples. The patient was discharged with a plan for outpatient chemotherapy and genetic counseling.
Conclusion: Given the rarity of PPCCC, our case highlights how increased clinical vigilance and prompt multidisciplinary efforts are essential for an accurate diagnosis, especially in younger patients to not delay management. Currently, there are no established management guidelines; however, initial treatment with surgical debulking followed by chemotherapy is often practiced.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


