Mathilde I Looman, Tessa F Blanken, Tim M Schoenmakers, Joyce E Reesen, Marieke Effting, Floris E Linnebank, Annemieke van Straten, Jan H Kamphuis, Jaap Lancee
{"title":"电话引导睡眠限制失眠:一项随机睡眠日记对照试验。","authors":"Mathilde I Looman, Tessa F Blanken, Tim M Schoenmakers, Joyce E Reesen, Marieke Effting, Floris E Linnebank, Annemieke van Straten, Jan H Kamphuis, Jaap Lancee","doi":"10.1159/000545138","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Insomnia is common, but access to its first-line treatment, cognitive behavioral therapy for insomnia (CBT-I), is limited. To explore a scalable alternative, we investigated the efficacy of sleep restriction therapy (SRT), a core component of CBT-I, delivered via telephone.</p><p><strong>Methods: </strong>In a randomized controlled trial, 147 adults with insomnia were allocated to 6 weeks of telephone-guided SRT (n = 76) or a sleep diary control group (n = 71). The SRT group received weekly supporting phone calls lasting 10-15 min. At baseline and posttest, we measured insomnia severity (primary outcome), sleep diary measures, anxiety symptoms, depressive symptoms, presleep arousal, sleep-safety behaviors, daytime sleepiness, and dysfunctional sleep-related cognitions (secondary outcomes). The SRT group repeated these measures at 3- and 6-month follow-ups.</p><p><strong>Results: </strong>Telephone-guided SRT showed large between-group effects on insomnia severity at posttest relative to the sleep diary control group (d = 1.52; p < 0.001). Based on intention-to-treat, 36 (47%) participants randomized to SRT achieved clinical improvement, and 23 (30%) achieved insomnia remission. We found medium-to-large between-group effects at posttest (d = 0.53-1.18) for all secondary outcomes except daytime sleepiness and total sleep time. At 3- and 6-month follow-ups, the primary and all secondary outcomes, including daytime sleepiness and total sleep time, improved relative to baseline within the SRT group (d = 0.50-1.93).</p><p><strong>Conclusion: </strong>This trial shows that telephone-guided SRT is an effective insomnia treatment requiring minimal therapist guidance. If direct comparisons with CBT-I corroborate these findings, SRT could be an interesting scalable alternative to CBT-I as a first-line insomnia treatment.</p><p><strong>Trial registry: </strong>NCT05548907.</p>","PeriodicalId":20744,"journal":{"name":"Psychotherapy and Psychosomatics","volume":" ","pages":"147-161"},"PeriodicalIF":17.4000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12060811/pdf/","citationCount":"0","resultStr":"{\"title\":\"Telephone-Guided Sleep Restriction for Insomnia: A Randomized Sleep Diary-Controlled Trial.\",\"authors\":\"Mathilde I Looman, Tessa F Blanken, Tim M Schoenmakers, Joyce E Reesen, Marieke Effting, Floris E Linnebank, Annemieke van Straten, Jan H Kamphuis, Jaap Lancee\",\"doi\":\"10.1159/000545138\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Insomnia is common, but access to its first-line treatment, cognitive behavioral therapy for insomnia (CBT-I), is limited. To explore a scalable alternative, we investigated the efficacy of sleep restriction therapy (SRT), a core component of CBT-I, delivered via telephone.</p><p><strong>Methods: </strong>In a randomized controlled trial, 147 adults with insomnia were allocated to 6 weeks of telephone-guided SRT (n = 76) or a sleep diary control group (n = 71). The SRT group received weekly supporting phone calls lasting 10-15 min. At baseline and posttest, we measured insomnia severity (primary outcome), sleep diary measures, anxiety symptoms, depressive symptoms, presleep arousal, sleep-safety behaviors, daytime sleepiness, and dysfunctional sleep-related cognitions (secondary outcomes). The SRT group repeated these measures at 3- and 6-month follow-ups.</p><p><strong>Results: </strong>Telephone-guided SRT showed large between-group effects on insomnia severity at posttest relative to the sleep diary control group (d = 1.52; p < 0.001). Based on intention-to-treat, 36 (47%) participants randomized to SRT achieved clinical improvement, and 23 (30%) achieved insomnia remission. We found medium-to-large between-group effects at posttest (d = 0.53-1.18) for all secondary outcomes except daytime sleepiness and total sleep time. At 3- and 6-month follow-ups, the primary and all secondary outcomes, including daytime sleepiness and total sleep time, improved relative to baseline within the SRT group (d = 0.50-1.93).</p><p><strong>Conclusion: </strong>This trial shows that telephone-guided SRT is an effective insomnia treatment requiring minimal therapist guidance. If direct comparisons with CBT-I corroborate these findings, SRT could be an interesting scalable alternative to CBT-I as a first-line insomnia treatment.</p><p><strong>Trial registry: </strong>NCT05548907.</p>\",\"PeriodicalId\":20744,\"journal\":{\"name\":\"Psychotherapy and Psychosomatics\",\"volume\":\" \",\"pages\":\"147-161\"},\"PeriodicalIF\":17.4000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12060811/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Psychotherapy and Psychosomatics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000545138\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Psychotherapy and Psychosomatics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000545138","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
Telephone-Guided Sleep Restriction for Insomnia: A Randomized Sleep Diary-Controlled Trial.
Introduction: Insomnia is common, but access to its first-line treatment, cognitive behavioral therapy for insomnia (CBT-I), is limited. To explore a scalable alternative, we investigated the efficacy of sleep restriction therapy (SRT), a core component of CBT-I, delivered via telephone.
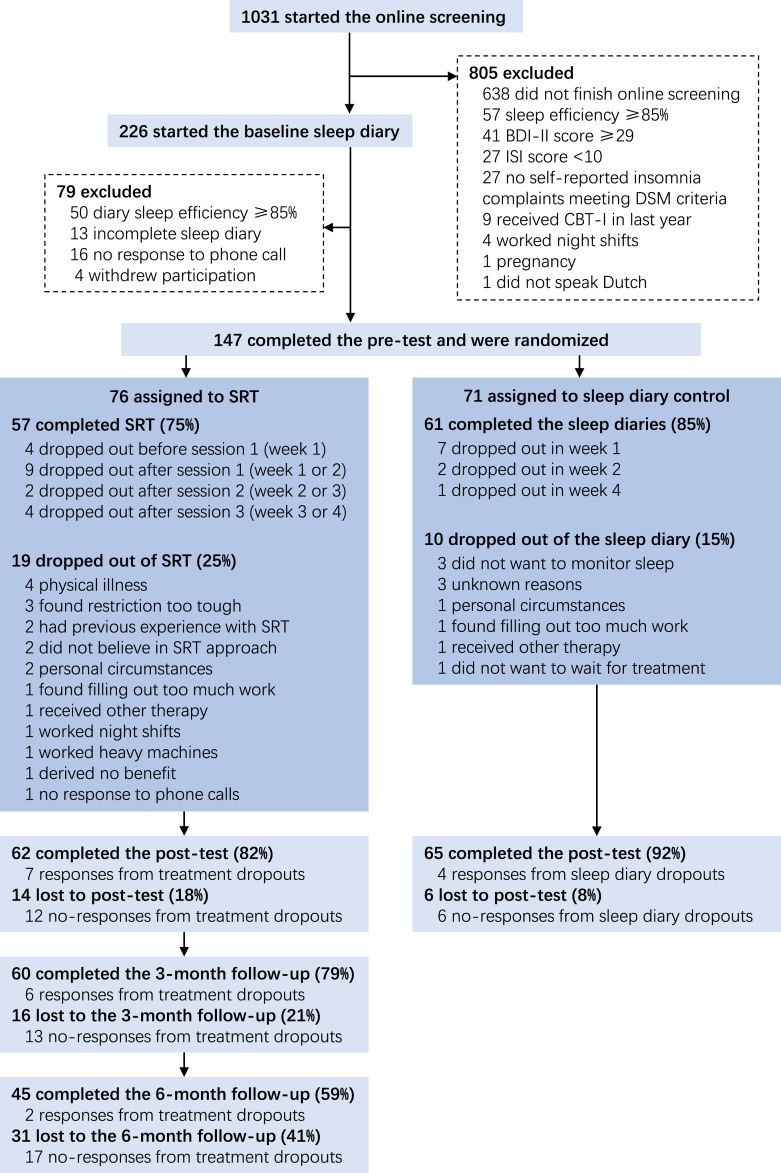
Methods: In a randomized controlled trial, 147 adults with insomnia were allocated to 6 weeks of telephone-guided SRT (n = 76) or a sleep diary control group (n = 71). The SRT group received weekly supporting phone calls lasting 10-15 min. At baseline and posttest, we measured insomnia severity (primary outcome), sleep diary measures, anxiety symptoms, depressive symptoms, presleep arousal, sleep-safety behaviors, daytime sleepiness, and dysfunctional sleep-related cognitions (secondary outcomes). The SRT group repeated these measures at 3- and 6-month follow-ups.
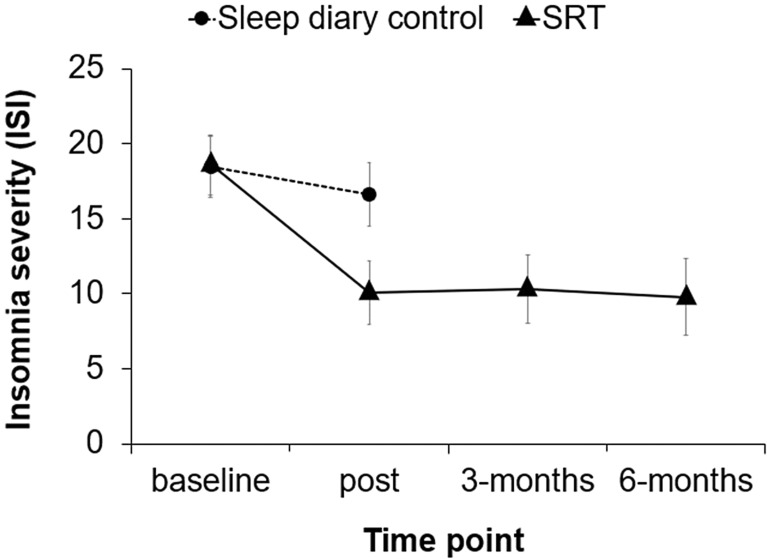
Results: Telephone-guided SRT showed large between-group effects on insomnia severity at posttest relative to the sleep diary control group (d = 1.52; p < 0.001). Based on intention-to-treat, 36 (47%) participants randomized to SRT achieved clinical improvement, and 23 (30%) achieved insomnia remission. We found medium-to-large between-group effects at posttest (d = 0.53-1.18) for all secondary outcomes except daytime sleepiness and total sleep time. At 3- and 6-month follow-ups, the primary and all secondary outcomes, including daytime sleepiness and total sleep time, improved relative to baseline within the SRT group (d = 0.50-1.93).
Conclusion: This trial shows that telephone-guided SRT is an effective insomnia treatment requiring minimal therapist guidance. If direct comparisons with CBT-I corroborate these findings, SRT could be an interesting scalable alternative to CBT-I as a first-line insomnia treatment.
期刊介绍:
Psychotherapy and Psychosomatics is a reputable journal that has been published since 1953. Over the years, it has gained recognition for its independence, originality, and methodological rigor. The journal has been at the forefront of research in psychosomatic medicine, psychotherapy research, and psychopharmacology, and has contributed to the development of new lines of research in these areas. It is now ranked among the world's most cited journals in the field.
As the official journal of the International College of Psychosomatic Medicine and the World Federation for Psychotherapy, Psychotherapy and Psychosomatics serves as a platform for discussing current and controversial issues and showcasing innovations in assessment and treatment. It offers a unique forum for cutting-edge thinking at the intersection of medical and behavioral sciences, catering to both practicing clinicians and researchers.
The journal is indexed in various databases and platforms such as PubMed, MEDLINE, Web of Science, Science Citation Index, Social Sciences Citation Index, Science Citation Index Expanded, BIOSIS Previews, Google Scholar, Academic Search, and Health Research Premium Collection, among others.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


