{"title":"慢性肾脏疾病对骨折术后并发症和死亡率的影响。","authors":"Bei-Bei Lu, Xu-Rui Liu, Qing-Song Chen, Xiao-Lin Yuan, Qian Luo, Yu-Dong Hu, Xiao-Hui Liao","doi":"10.1186/s13741-025-00514-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The purpose of this meta-analysis was to evaluate the effects of CKD on postoperative complications and the survival of patients with fractures.</p><p><strong>Methods: </strong>The PubMed, Embase, Cochrane Library, and CNKI databases were searched from inception to May 15, 2024. The search strategy focused on two keywords: dialysis and hip fracture. Pooled odds ratios and mean differences were analyzed. RevMan 5.4 was used for data analysis in this meta-analysis.</p><p><strong>Results: </strong>This meta-analysis included 19 studies involving 1,615,440 patients. The CKD group had higher proportions of males, smokers, and patients with preoperative comorbidities such as diabetes, hypertension, heart failure, chronic lung disease, coronary heart disease, peripheral vascular disease, dementia, and wound infection. The CKD group also had a greater likelihood of postoperative myocardial infarction (OR = 1.67, 95% CI = 1.54-1.81, P < 0.00001, I<sup>2</sup> = 33%). There was no significant difference in cerebrovascular accidents, liver failure, sepsis, and overall complications between the two groups. Additionally, the CKD group had higher mortality rates at 30 days (OR = 2.71, 95% CI = 2.23-3.28, P < 0.00001, I<sup>2</sup> = 84%), 1 year (OR = 3.17, 95% CI = 2.64-3.82, P < 0.00001, I<sup>2</sup> = 85%), 2 years (OR = 3.06, 95% CI = 2.88-3.25, P < 0.00001, I<sup>2</sup> = 8%), and 10 years (OR = 6.85, 95% CI = 5.84-8.03, P < 0.00001, I<sup>2</sup> = 0%) post-surgery compared to the non-CKD group.</p><p><strong>Conclusion: </strong>Compared with patients in the non-CKD group, patients in the CKD group did not significantly differ in the incidence of most postoperative complications after fracture surgery. However, the CKD group had a significantly greater incidence of myocardial infarction and markedly higher postoperative mortality rates at 30 days, 1 year, 2 years, and 10 years.</p><p><strong>Trial registration: </strong>PROSPERO CRD42025648208.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"14 1","pages":"34"},"PeriodicalIF":2.1000,"publicationDate":"2025-03-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11929312/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of chronic kidney disease on complications and mortality after fracture surgery.\",\"authors\":\"Bei-Bei Lu, Xu-Rui Liu, Qing-Song Chen, Xiao-Lin Yuan, Qian Luo, Yu-Dong Hu, Xiao-Hui Liao\",\"doi\":\"10.1186/s13741-025-00514-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The purpose of this meta-analysis was to evaluate the effects of CKD on postoperative complications and the survival of patients with fractures.</p><p><strong>Methods: </strong>The PubMed, Embase, Cochrane Library, and CNKI databases were searched from inception to May 15, 2024. The search strategy focused on two keywords: dialysis and hip fracture. Pooled odds ratios and mean differences were analyzed. RevMan 5.4 was used for data analysis in this meta-analysis.</p><p><strong>Results: </strong>This meta-analysis included 19 studies involving 1,615,440 patients. The CKD group had higher proportions of males, smokers, and patients with preoperative comorbidities such as diabetes, hypertension, heart failure, chronic lung disease, coronary heart disease, peripheral vascular disease, dementia, and wound infection. The CKD group also had a greater likelihood of postoperative myocardial infarction (OR = 1.67, 95% CI = 1.54-1.81, P < 0.00001, I<sup>2</sup> = 33%). There was no significant difference in cerebrovascular accidents, liver failure, sepsis, and overall complications between the two groups. Additionally, the CKD group had higher mortality rates at 30 days (OR = 2.71, 95% CI = 2.23-3.28, P < 0.00001, I<sup>2</sup> = 84%), 1 year (OR = 3.17, 95% CI = 2.64-3.82, P < 0.00001, I<sup>2</sup> = 85%), 2 years (OR = 3.06, 95% CI = 2.88-3.25, P < 0.00001, I<sup>2</sup> = 8%), and 10 years (OR = 6.85, 95% CI = 5.84-8.03, P < 0.00001, I<sup>2</sup> = 0%) post-surgery compared to the non-CKD group.</p><p><strong>Conclusion: </strong>Compared with patients in the non-CKD group, patients in the CKD group did not significantly differ in the incidence of most postoperative complications after fracture surgery. However, the CKD group had a significantly greater incidence of myocardial infarction and markedly higher postoperative mortality rates at 30 days, 1 year, 2 years, and 10 years.</p><p><strong>Trial registration: </strong>PROSPERO CRD42025648208.</p>\",\"PeriodicalId\":19764,\"journal\":{\"name\":\"Perioperative Medicine\",\"volume\":\"14 1\",\"pages\":\"34\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-03-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11929312/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Perioperative Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13741-025-00514-y\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-025-00514-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Effects of chronic kidney disease on complications and mortality after fracture surgery.
Purpose: The purpose of this meta-analysis was to evaluate the effects of CKD on postoperative complications and the survival of patients with fractures.
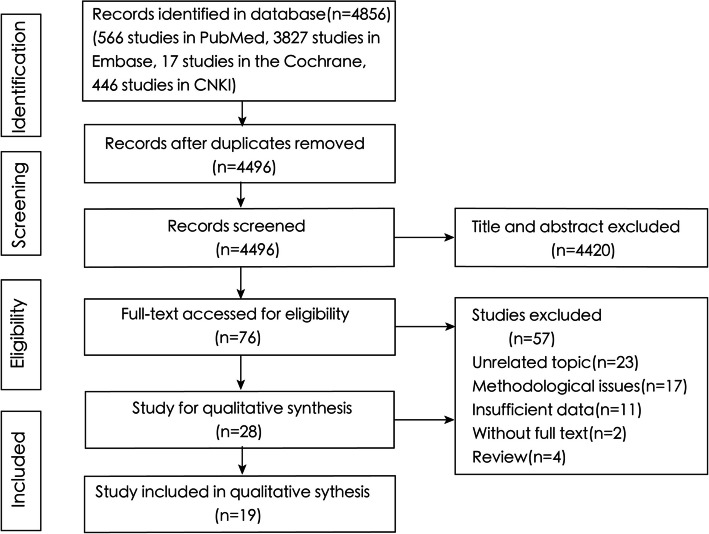
Methods: The PubMed, Embase, Cochrane Library, and CNKI databases were searched from inception to May 15, 2024. The search strategy focused on two keywords: dialysis and hip fracture. Pooled odds ratios and mean differences were analyzed. RevMan 5.4 was used for data analysis in this meta-analysis.
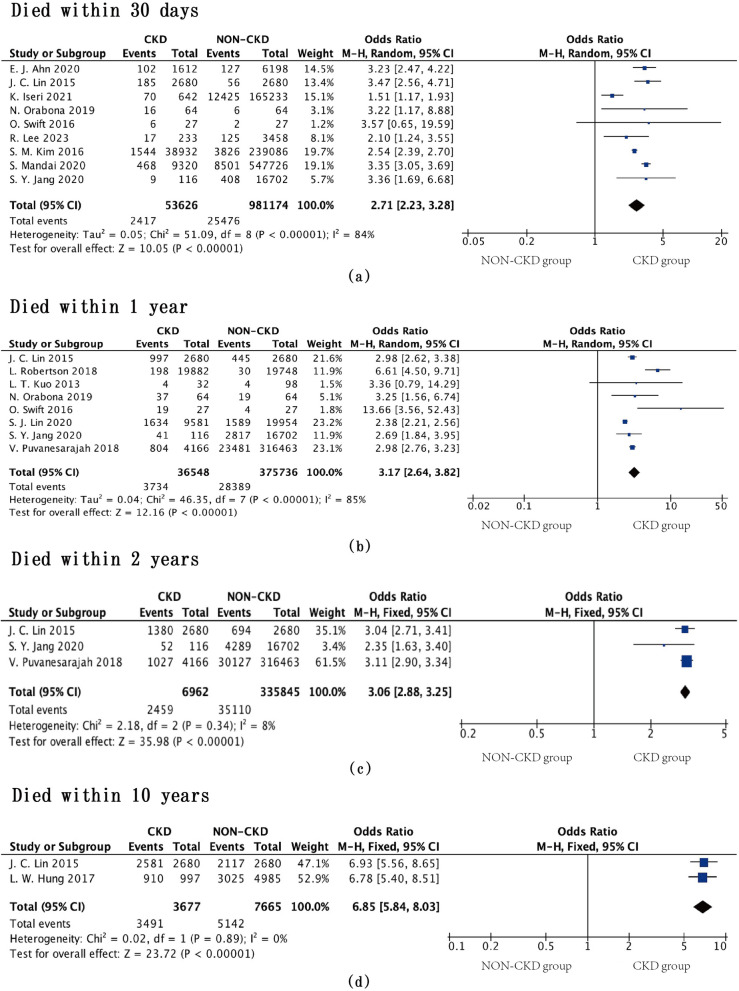
Results: This meta-analysis included 19 studies involving 1,615,440 patients. The CKD group had higher proportions of males, smokers, and patients with preoperative comorbidities such as diabetes, hypertension, heart failure, chronic lung disease, coronary heart disease, peripheral vascular disease, dementia, and wound infection. The CKD group also had a greater likelihood of postoperative myocardial infarction (OR = 1.67, 95% CI = 1.54-1.81, P < 0.00001, I2 = 33%). There was no significant difference in cerebrovascular accidents, liver failure, sepsis, and overall complications between the two groups. Additionally, the CKD group had higher mortality rates at 30 days (OR = 2.71, 95% CI = 2.23-3.28, P < 0.00001, I2 = 84%), 1 year (OR = 3.17, 95% CI = 2.64-3.82, P < 0.00001, I2 = 85%), 2 years (OR = 3.06, 95% CI = 2.88-3.25, P < 0.00001, I2 = 8%), and 10 years (OR = 6.85, 95% CI = 5.84-8.03, P < 0.00001, I2 = 0%) post-surgery compared to the non-CKD group.
Conclusion: Compared with patients in the non-CKD group, patients in the CKD group did not significantly differ in the incidence of most postoperative complications after fracture surgery. However, the CKD group had a significantly greater incidence of myocardial infarction and markedly higher postoperative mortality rates at 30 days, 1 year, 2 years, and 10 years.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


