{"title":"基于机器学习的重症肺炎全因死亡率预测模型","authors":"Weichao Zhao, Xuyan Li, Lianjun Gao, Zhuang Ai, Yaping Lu, Jiachen Li, Dong Wang, Xinlou Li, Nan Song, Xuan Huang, Zhao-Hui Tong","doi":"10.1136/bmjresp-2023-001983","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Severe pneumonia has a poor prognosis and high mortality. Current severity scores such as Acute Physiology and Chronic Health Evaluation (APACHE-II) and Sequential Organ Failure Assessment (SOFA), have limited ability to help clinicians in classification and management decisions. The goal of this study was to analyse the clinical characteristics of severe pneumonia and develop a machine learning-based mortality-prediction model for patients with severe pneumonia.</p><p><strong>Methods: </strong>Consecutive patients with severe pneumonia between 2013 and 2022 admitted to Beijing Chaoyang Hospital affiliated with Capital Medical University were included. In-hospital all-cause mortality was the outcome of this study. We performed a retrospective analysis of the cohort, stratifying patients into survival and non-survival groups, using mainstream machine learning algorithms (light gradient boosting machine, support vector classifier and random forest). We aimed to construct a mortality-prediction model for patients with severe pneumonia based on their accessible clinical and laboratory data. The discriminative ability was evaluated using the area under the receiver operating characteristic curve (AUC). The calibration curve was used to assess the fit goodness of the model, and decision curve analysis was performed to quantify clinical utility. By means of logistic regression, independent risk factors for death in severe pneumonia were figured out to provide an important basis for clinical decision-making.</p><p><strong>Results: </strong>A total of 875 patients were included in the development and validation cohorts, with the in-hospital mortality rate of 14.6%. The AUC of the model in the internal validation set was 0.8779 (95% CI, 0.738 to 0.974), showing a competitive discrimination ability that outperformed those of traditional clinical scoring systems, that is, APACHE-II, SOFA, CURB-65 (confusion, urea, respiratory rate, blood pressure, age ≥65 years), Pneumonia Severity Index. The calibration curve showed that the in-hospital mortality in severe pneumonia predicted by the model fit reasonably with the actual hospital mortality. In addition, the decision curve showed that the net clinical benefit was positive in both training and validation sets of hospitalised patients with severe pneumonia. Based on ensemble machine learning algorithms and logistic regression technique, the level of ferritin, lactic acid, blood urea nitrogen, creatine kinase, eosinophil and the requirement of vasopressors were identified as top independent predictors of in-hospital mortality with severe pneumonia.</p><p><strong>Conclusion: </strong>A robust clinical model for predicting the risk of in-hospital mortality after severe pneumonia was successfully developed using machine learning techniques. The performance of this model demonstrates the effectiveness of these techniques in creating accurate predictive models, and the use of this model has the potential to greatly assist patients and clinical doctors in making well-informed decisions regarding patient care.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-03-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11934410/pdf/","citationCount":"0","resultStr":"{\"title\":\"Machine learning-based model for predicting all-cause mortality in severe pneumonia.\",\"authors\":\"Weichao Zhao, Xuyan Li, Lianjun Gao, Zhuang Ai, Yaping Lu, Jiachen Li, Dong Wang, Xinlou Li, Nan Song, Xuan Huang, Zhao-Hui Tong\",\"doi\":\"10.1136/bmjresp-2023-001983\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Severe pneumonia has a poor prognosis and high mortality. Current severity scores such as Acute Physiology and Chronic Health Evaluation (APACHE-II) and Sequential Organ Failure Assessment (SOFA), have limited ability to help clinicians in classification and management decisions. The goal of this study was to analyse the clinical characteristics of severe pneumonia and develop a machine learning-based mortality-prediction model for patients with severe pneumonia.</p><p><strong>Methods: </strong>Consecutive patients with severe pneumonia between 2013 and 2022 admitted to Beijing Chaoyang Hospital affiliated with Capital Medical University were included. In-hospital all-cause mortality was the outcome of this study. We performed a retrospective analysis of the cohort, stratifying patients into survival and non-survival groups, using mainstream machine learning algorithms (light gradient boosting machine, support vector classifier and random forest). We aimed to construct a mortality-prediction model for patients with severe pneumonia based on their accessible clinical and laboratory data. The discriminative ability was evaluated using the area under the receiver operating characteristic curve (AUC). The calibration curve was used to assess the fit goodness of the model, and decision curve analysis was performed to quantify clinical utility. By means of logistic regression, independent risk factors for death in severe pneumonia were figured out to provide an important basis for clinical decision-making.</p><p><strong>Results: </strong>A total of 875 patients were included in the development and validation cohorts, with the in-hospital mortality rate of 14.6%. The AUC of the model in the internal validation set was 0.8779 (95% CI, 0.738 to 0.974), showing a competitive discrimination ability that outperformed those of traditional clinical scoring systems, that is, APACHE-II, SOFA, CURB-65 (confusion, urea, respiratory rate, blood pressure, age ≥65 years), Pneumonia Severity Index. The calibration curve showed that the in-hospital mortality in severe pneumonia predicted by the model fit reasonably with the actual hospital mortality. In addition, the decision curve showed that the net clinical benefit was positive in both training and validation sets of hospitalised patients with severe pneumonia. Based on ensemble machine learning algorithms and logistic regression technique, the level of ferritin, lactic acid, blood urea nitrogen, creatine kinase, eosinophil and the requirement of vasopressors were identified as top independent predictors of in-hospital mortality with severe pneumonia.</p><p><strong>Conclusion: </strong>A robust clinical model for predicting the risk of in-hospital mortality after severe pneumonia was successfully developed using machine learning techniques. The performance of this model demonstrates the effectiveness of these techniques in creating accurate predictive models, and the use of this model has the potential to greatly assist patients and clinical doctors in making well-informed decisions regarding patient care.</p>\",\"PeriodicalId\":9048,\"journal\":{\"name\":\"BMJ Open Respiratory Research\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-03-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11934410/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjresp-2023-001983\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2023-001983","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Machine learning-based model for predicting all-cause mortality in severe pneumonia.
Background: Severe pneumonia has a poor prognosis and high mortality. Current severity scores such as Acute Physiology and Chronic Health Evaluation (APACHE-II) and Sequential Organ Failure Assessment (SOFA), have limited ability to help clinicians in classification and management decisions. The goal of this study was to analyse the clinical characteristics of severe pneumonia and develop a machine learning-based mortality-prediction model for patients with severe pneumonia.
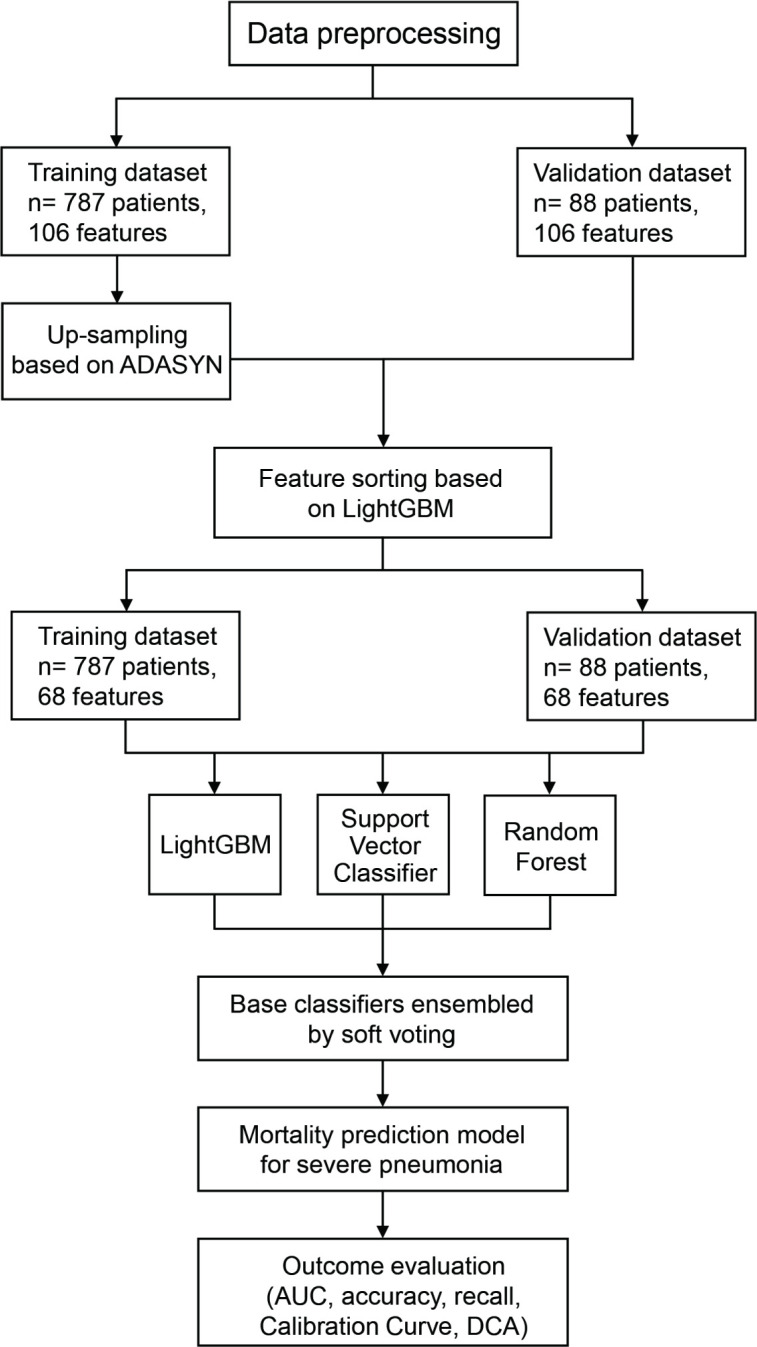
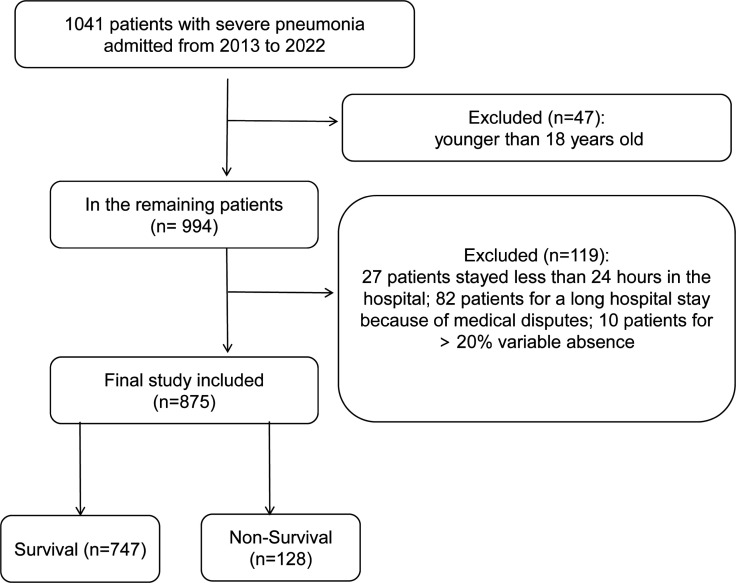
Methods: Consecutive patients with severe pneumonia between 2013 and 2022 admitted to Beijing Chaoyang Hospital affiliated with Capital Medical University were included. In-hospital all-cause mortality was the outcome of this study. We performed a retrospective analysis of the cohort, stratifying patients into survival and non-survival groups, using mainstream machine learning algorithms (light gradient boosting machine, support vector classifier and random forest). We aimed to construct a mortality-prediction model for patients with severe pneumonia based on their accessible clinical and laboratory data. The discriminative ability was evaluated using the area under the receiver operating characteristic curve (AUC). The calibration curve was used to assess the fit goodness of the model, and decision curve analysis was performed to quantify clinical utility. By means of logistic regression, independent risk factors for death in severe pneumonia were figured out to provide an important basis for clinical decision-making.
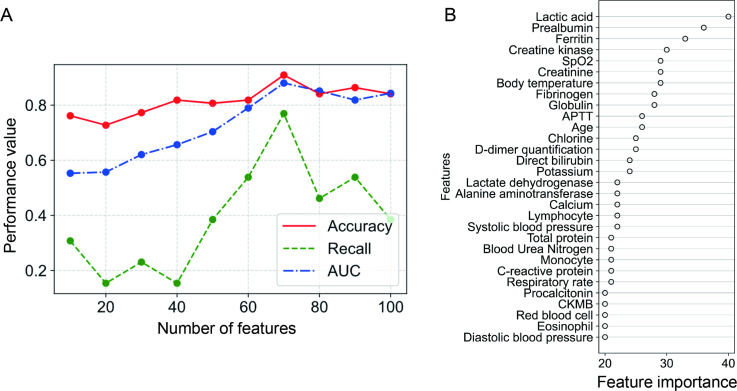
Results: A total of 875 patients were included in the development and validation cohorts, with the in-hospital mortality rate of 14.6%. The AUC of the model in the internal validation set was 0.8779 (95% CI, 0.738 to 0.974), showing a competitive discrimination ability that outperformed those of traditional clinical scoring systems, that is, APACHE-II, SOFA, CURB-65 (confusion, urea, respiratory rate, blood pressure, age ≥65 years), Pneumonia Severity Index. The calibration curve showed that the in-hospital mortality in severe pneumonia predicted by the model fit reasonably with the actual hospital mortality. In addition, the decision curve showed that the net clinical benefit was positive in both training and validation sets of hospitalised patients with severe pneumonia. Based on ensemble machine learning algorithms and logistic regression technique, the level of ferritin, lactic acid, blood urea nitrogen, creatine kinase, eosinophil and the requirement of vasopressors were identified as top independent predictors of in-hospital mortality with severe pneumonia.
Conclusion: A robust clinical model for predicting the risk of in-hospital mortality after severe pneumonia was successfully developed using machine learning techniques. The performance of this model demonstrates the effectiveness of these techniques in creating accurate predictive models, and the use of this model has the potential to greatly assist patients and clinical doctors in making well-informed decisions regarding patient care.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


