Helena Rocha, Rita Gouveia, Catarina Elias, Catarina Reis, Ana Margarida Fonseca, Adriana Costa, Carolina Guimarães, Rui Ribeiro, Ana Toste, Carlos Grijó, Helena Reis, Ana Neves, Jorge Almeida, Patrícia Lourenço
{"title":"慢性心力衰竭患者收缩压升高与生存优势相关。","authors":"Helena Rocha, Rita Gouveia, Catarina Elias, Catarina Reis, Ana Margarida Fonseca, Adriana Costa, Carolina Guimarães, Rui Ribeiro, Ana Toste, Carlos Grijó, Helena Reis, Ana Neves, Jorge Almeida, Patrícia Lourenço","doi":"10.1097/j.pbj.0000000000000284","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The impact of systolic blood pressure (SBP) variation on chronic heart failure (HF) is largely unknown. We assessed the impact of SBP variation in patients with chronic HF.</p><p><strong>Methods: </strong>This is a retrospective analysis of adult ambulatory patients with HF with left ventricular systolic dysfunction (LVSD). SBP variation = SBP at the index visit - SBP at the 1-year visit. Patients dying in the first year or with missing data concerning SBP were excluded. Patients with SBP increase ≥10 mmHg during the first year were compared with the remaining. Determinants of SBP increase were assessed by binary logistic regression analysis. The patients were followed up from the 1-year visit up to 5 years. The primary end point was all-cause mortality. A Cox regression analysis was used to determine the association of SBP variation with mortality.</p><p><strong>Results: </strong>We studied 787 patients (68% male), with a mean age of 70 years. SBP increased by ≥10 mmHg in 277 patients (35.2%) and remained stable or decreased in 510. Patients in whom SBP increased more often presented severe LVSD and nonischemic HF; they had lower baseline SBP and were more medicated with loop diuretics. Independent predictors of SBP increase were lower basal SBP and loop diuretic use. Patients with a SBP increase ≥10 mmHg had a crude hazard ratio (HR) of all-cause mortality of 0.74 (0.59-0.94), and the multivariate-adjusted HR was 0.61 (0.46-0.79).</p><p><strong>Conclusions: </strong>Patients with chronic HF with SBP increase ≥10 mmHg over the first year have a 39% reduction in the all-cause mortality risk irrespective of basal SBP, severity of ventricular dysfunction, and evidence-based drug use. Patients with SBP stability or decrease have a similarly poor prognosis.</p>","PeriodicalId":74479,"journal":{"name":"Porto biomedical journal","volume":"10 2","pages":"e284"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11913415/pdf/","citationCount":"0","resultStr":"{\"title\":\"Systolic blood pressure increase in chronic heart failure associates with survival advantage.\",\"authors\":\"Helena Rocha, Rita Gouveia, Catarina Elias, Catarina Reis, Ana Margarida Fonseca, Adriana Costa, Carolina Guimarães, Rui Ribeiro, Ana Toste, Carlos Grijó, Helena Reis, Ana Neves, Jorge Almeida, Patrícia Lourenço\",\"doi\":\"10.1097/j.pbj.0000000000000284\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The impact of systolic blood pressure (SBP) variation on chronic heart failure (HF) is largely unknown. We assessed the impact of SBP variation in patients with chronic HF.</p><p><strong>Methods: </strong>This is a retrospective analysis of adult ambulatory patients with HF with left ventricular systolic dysfunction (LVSD). SBP variation = SBP at the index visit - SBP at the 1-year visit. Patients dying in the first year or with missing data concerning SBP were excluded. Patients with SBP increase ≥10 mmHg during the first year were compared with the remaining. Determinants of SBP increase were assessed by binary logistic regression analysis. The patients were followed up from the 1-year visit up to 5 years. The primary end point was all-cause mortality. A Cox regression analysis was used to determine the association of SBP variation with mortality.</p><p><strong>Results: </strong>We studied 787 patients (68% male), with a mean age of 70 years. SBP increased by ≥10 mmHg in 277 patients (35.2%) and remained stable or decreased in 510. Patients in whom SBP increased more often presented severe LVSD and nonischemic HF; they had lower baseline SBP and were more medicated with loop diuretics. Independent predictors of SBP increase were lower basal SBP and loop diuretic use. Patients with a SBP increase ≥10 mmHg had a crude hazard ratio (HR) of all-cause mortality of 0.74 (0.59-0.94), and the multivariate-adjusted HR was 0.61 (0.46-0.79).</p><p><strong>Conclusions: </strong>Patients with chronic HF with SBP increase ≥10 mmHg over the first year have a 39% reduction in the all-cause mortality risk irrespective of basal SBP, severity of ventricular dysfunction, and evidence-based drug use. Patients with SBP stability or decrease have a similarly poor prognosis.</p>\",\"PeriodicalId\":74479,\"journal\":{\"name\":\"Porto biomedical journal\",\"volume\":\"10 2\",\"pages\":\"e284\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11913415/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Porto biomedical journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/j.pbj.0000000000000284\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Porto biomedical journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/j.pbj.0000000000000284","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Systolic blood pressure increase in chronic heart failure associates with survival advantage.
Background: The impact of systolic blood pressure (SBP) variation on chronic heart failure (HF) is largely unknown. We assessed the impact of SBP variation in patients with chronic HF.
Methods: This is a retrospective analysis of adult ambulatory patients with HF with left ventricular systolic dysfunction (LVSD). SBP variation = SBP at the index visit - SBP at the 1-year visit. Patients dying in the first year or with missing data concerning SBP were excluded. Patients with SBP increase ≥10 mmHg during the first year were compared with the remaining. Determinants of SBP increase were assessed by binary logistic regression analysis. The patients were followed up from the 1-year visit up to 5 years. The primary end point was all-cause mortality. A Cox regression analysis was used to determine the association of SBP variation with mortality.
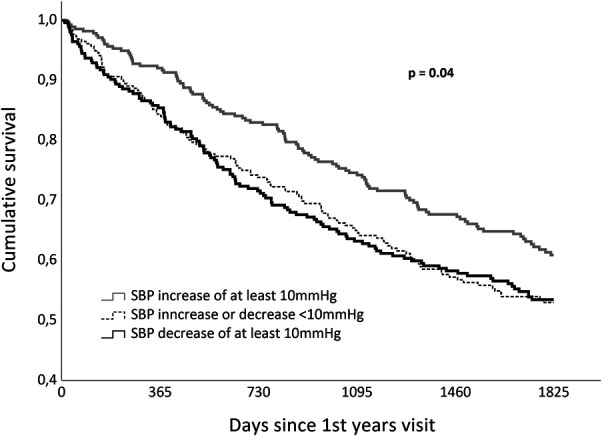
Results: We studied 787 patients (68% male), with a mean age of 70 years. SBP increased by ≥10 mmHg in 277 patients (35.2%) and remained stable or decreased in 510. Patients in whom SBP increased more often presented severe LVSD and nonischemic HF; they had lower baseline SBP and were more medicated with loop diuretics. Independent predictors of SBP increase were lower basal SBP and loop diuretic use. Patients with a SBP increase ≥10 mmHg had a crude hazard ratio (HR) of all-cause mortality of 0.74 (0.59-0.94), and the multivariate-adjusted HR was 0.61 (0.46-0.79).
Conclusions: Patients with chronic HF with SBP increase ≥10 mmHg over the first year have a 39% reduction in the all-cause mortality risk irrespective of basal SBP, severity of ventricular dysfunction, and evidence-based drug use. Patients with SBP stability or decrease have a similarly poor prognosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


