{"title":"ustekinumab治疗Takayasu动脉炎的3期多中心、随机、双盲、安慰剂对照、平行组研究","authors":"Hajime Yoshifuji, Tomonori Ishii, Hiroki Ohashi, Katsunori Yoshizawa, Maki Mihoya, Kazuko Nishikawa, Yoshikazu Nakaoka","doi":"10.1093/rap/rkaf013","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Takayasu arteritis (TAK) is a rare, chronic large vessel vasculitis with unmet treatment needs. This phase 3 study aimed to evaluate efficacy, safety, pharmacokinetics and immunogenicity of ustekinumab (UST) in Japanese patients with TAK.</p><p><strong>Methods: </strong>Patients with TAK who had relapsed ≤12 weeks prior to study intervention administration and achieved remission thereafter with standard-of-care including corticosteroid intensification were randomized 1:1 to receive UST or matching placebo with protocol-defined oral glucocorticoid taper regimen. The double-blind (DB) phase was up to the patient's relapse/total of 35 relapse events, followed by the open-label extension (OLE) phase. Primary endpoint was the time to relapse of TAK per protocol-defined criteria through the end of the DB phase.</p><p><strong>Results: </strong>The study was terminated early due to patient recruitment challenge. Of 14 patients randomized, 8 relapsed during the DB phase (UST: 4/6; placebo: 4/8). The median time to relapse (weeks) was 11.14 (95% CI: 4.14, not estimated [NE]) for UST and 12.64 (95% confidence interval [CI]: 12.14, NE) for placebo (hazard ratio [HR] = 1.86 [95% CI: 0.41, 8.47]). In the DB phase, one patient in each group reported serious adverse event (SAE; UST: vascular pseudoaneurysm and brachiocephalic artery stenosis; placebo: cholecystitis); none were related to study intervention. Through the OLE phase, 1/4 (25.0%) patients in the UST-UST group (vascular graft infection considered related to study intervention) and none in the placebo-UST had SAEs. There were no serious infections/deaths throughout the study.</p><p><strong>Conclusion: </strong>The efficacy of UST in patients with TAK cannot be adequately assessed as the pre-determined sample size was not reached, and the study was prematurely terminated. No new safety signal of UST was identified.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov, https://clinicaltrials.gov, NCT04882072; jrct.niph.go.jp, https://jrct.niph.go.jp, jRCT2061210007; Clinical Registry, CR108981.</p>","PeriodicalId":21350,"journal":{"name":"Rheumatology Advances in Practice","volume":"9 2","pages":"rkaf013"},"PeriodicalIF":2.1000,"publicationDate":"2025-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11919447/pdf/","citationCount":"0","resultStr":"{\"title\":\"Phase 3, multicentre, randomized, double-blind, placebo-controlled, parallel-group study of ustekinumab in patients with Takayasu arteritis.\",\"authors\":\"Hajime Yoshifuji, Tomonori Ishii, Hiroki Ohashi, Katsunori Yoshizawa, Maki Mihoya, Kazuko Nishikawa, Yoshikazu Nakaoka\",\"doi\":\"10.1093/rap/rkaf013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Takayasu arteritis (TAK) is a rare, chronic large vessel vasculitis with unmet treatment needs. This phase 3 study aimed to evaluate efficacy, safety, pharmacokinetics and immunogenicity of ustekinumab (UST) in Japanese patients with TAK.</p><p><strong>Methods: </strong>Patients with TAK who had relapsed ≤12 weeks prior to study intervention administration and achieved remission thereafter with standard-of-care including corticosteroid intensification were randomized 1:1 to receive UST or matching placebo with protocol-defined oral glucocorticoid taper regimen. The double-blind (DB) phase was up to the patient's relapse/total of 35 relapse events, followed by the open-label extension (OLE) phase. Primary endpoint was the time to relapse of TAK per protocol-defined criteria through the end of the DB phase.</p><p><strong>Results: </strong>The study was terminated early due to patient recruitment challenge. Of 14 patients randomized, 8 relapsed during the DB phase (UST: 4/6; placebo: 4/8). The median time to relapse (weeks) was 11.14 (95% CI: 4.14, not estimated [NE]) for UST and 12.64 (95% confidence interval [CI]: 12.14, NE) for placebo (hazard ratio [HR] = 1.86 [95% CI: 0.41, 8.47]). In the DB phase, one patient in each group reported serious adverse event (SAE; UST: vascular pseudoaneurysm and brachiocephalic artery stenosis; placebo: cholecystitis); none were related to study intervention. Through the OLE phase, 1/4 (25.0%) patients in the UST-UST group (vascular graft infection considered related to study intervention) and none in the placebo-UST had SAEs. There were no serious infections/deaths throughout the study.</p><p><strong>Conclusion: </strong>The efficacy of UST in patients with TAK cannot be adequately assessed as the pre-determined sample size was not reached, and the study was prematurely terminated. No new safety signal of UST was identified.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov, https://clinicaltrials.gov, NCT04882072; jrct.niph.go.jp, https://jrct.niph.go.jp, jRCT2061210007; Clinical Registry, CR108981.</p>\",\"PeriodicalId\":21350,\"journal\":{\"name\":\"Rheumatology Advances in Practice\",\"volume\":\"9 2\",\"pages\":\"rkaf013\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-02-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11919447/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rheumatology Advances in Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/rap/rkaf013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rheumatology Advances in Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/rap/rkaf013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Phase 3, multicentre, randomized, double-blind, placebo-controlled, parallel-group study of ustekinumab in patients with Takayasu arteritis.
Objectives: Takayasu arteritis (TAK) is a rare, chronic large vessel vasculitis with unmet treatment needs. This phase 3 study aimed to evaluate efficacy, safety, pharmacokinetics and immunogenicity of ustekinumab (UST) in Japanese patients with TAK.
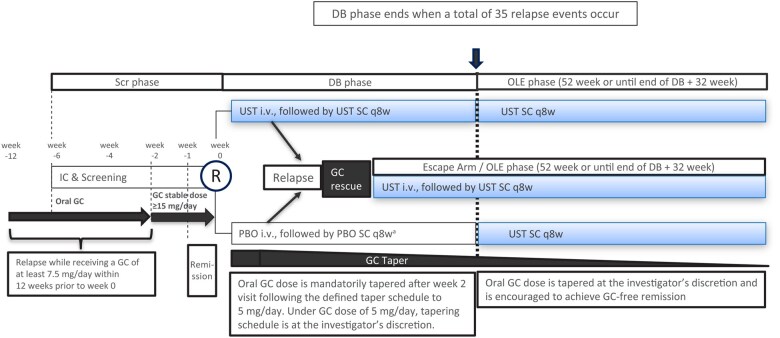
Methods: Patients with TAK who had relapsed ≤12 weeks prior to study intervention administration and achieved remission thereafter with standard-of-care including corticosteroid intensification were randomized 1:1 to receive UST or matching placebo with protocol-defined oral glucocorticoid taper regimen. The double-blind (DB) phase was up to the patient's relapse/total of 35 relapse events, followed by the open-label extension (OLE) phase. Primary endpoint was the time to relapse of TAK per protocol-defined criteria through the end of the DB phase.
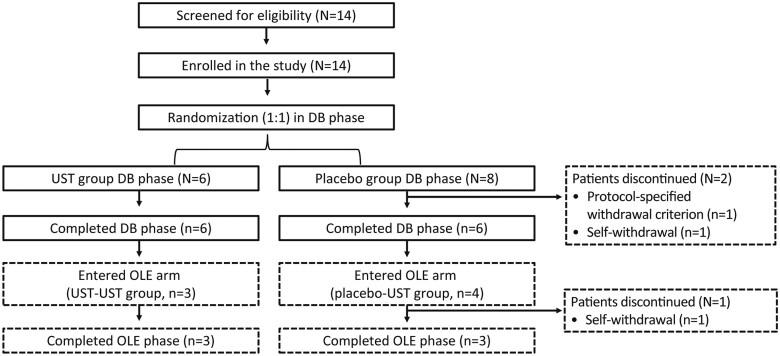
Results: The study was terminated early due to patient recruitment challenge. Of 14 patients randomized, 8 relapsed during the DB phase (UST: 4/6; placebo: 4/8). The median time to relapse (weeks) was 11.14 (95% CI: 4.14, not estimated [NE]) for UST and 12.64 (95% confidence interval [CI]: 12.14, NE) for placebo (hazard ratio [HR] = 1.86 [95% CI: 0.41, 8.47]). In the DB phase, one patient in each group reported serious adverse event (SAE; UST: vascular pseudoaneurysm and brachiocephalic artery stenosis; placebo: cholecystitis); none were related to study intervention. Through the OLE phase, 1/4 (25.0%) patients in the UST-UST group (vascular graft infection considered related to study intervention) and none in the placebo-UST had SAEs. There were no serious infections/deaths throughout the study.
Conclusion: The efficacy of UST in patients with TAK cannot be adequately assessed as the pre-determined sample size was not reached, and the study was prematurely terminated. No new safety signal of UST was identified.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


