{"title":"骨转移瘤切除和假体内重建后的患者生存率:一项单一肿瘤机构的全国性队列研究。","authors":"Aljaz Mercun, David Martincic, Blaz Mavcic","doi":"10.2478/raon-2025-0009","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of this nation-wide 2009-2021 cohort study was to analyze postoperative survival of patients with resected appendicular skeletal metastases and endoprosthetic reconstruction in comparison to sarcoma patients and non-oncological reconstructions.</p><p><strong>Patients and methods: </strong>A single institution nation-wide cohort of 144 consecutive patients with tumor endoprosthetic reconstructions (32 resected metastases, 73 resected sarcomas, 39 non-oncological) were stratified into histopathological groups according to the 2013-SPRING prediction model. Their survival was analyzed with the Kaplan-Meier method and Cox regression.</p><p><strong>Results: </strong>The observed patient survival rates after wide resection of fast/moderate/slow growing metastases were 25/55/88% at 2 years and 10/30/83% at 5 years, while in sarcomas the observed survival rates were 80% at 2 years and 69% at 5 years. Estimated mean postoperative survival after resection of skeletal metastases was significantly shorter in comparison to sarcomas (4.6 years vs. 9.1 years, log-rank p < 0.001). Predictors of worse patient survival included higher age, pathologic fracture or >1 metastasis, diagnostic group fast-growing metastases and higher preoperative C-reactive protein (CRP).</p><p><strong>Conclusions: </strong>Wide resection and endoprosthetic reconstruction offer a reliable solution in selected patients with skeletal metastases. Higher age, fast-growing metastases (from bladder cancer, colorectal, hepatocellular, lung cancer, malignant melanoma, unknown origin), pathologic fracture or >1 metastasis and elevated CRP predict shorter patient survival and may represent a relative contraindication in this regard.</p>","PeriodicalId":21034,"journal":{"name":"Radiology and Oncology","volume":" ","pages":"450-456"},"PeriodicalIF":2.2000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12441881/pdf/","citationCount":"0","resultStr":"{\"title\":\"Patient survival after resection of skeletal metastases and endoprosthetic reconstruction: a nation-wide cohort study in a single oncological institution.\",\"authors\":\"Aljaz Mercun, David Martincic, Blaz Mavcic\",\"doi\":\"10.2478/raon-2025-0009\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The aim of this nation-wide 2009-2021 cohort study was to analyze postoperative survival of patients with resected appendicular skeletal metastases and endoprosthetic reconstruction in comparison to sarcoma patients and non-oncological reconstructions.</p><p><strong>Patients and methods: </strong>A single institution nation-wide cohort of 144 consecutive patients with tumor endoprosthetic reconstructions (32 resected metastases, 73 resected sarcomas, 39 non-oncological) were stratified into histopathological groups according to the 2013-SPRING prediction model. Their survival was analyzed with the Kaplan-Meier method and Cox regression.</p><p><strong>Results: </strong>The observed patient survival rates after wide resection of fast/moderate/slow growing metastases were 25/55/88% at 2 years and 10/30/83% at 5 years, while in sarcomas the observed survival rates were 80% at 2 years and 69% at 5 years. Estimated mean postoperative survival after resection of skeletal metastases was significantly shorter in comparison to sarcomas (4.6 years vs. 9.1 years, log-rank p < 0.001). Predictors of worse patient survival included higher age, pathologic fracture or >1 metastasis, diagnostic group fast-growing metastases and higher preoperative C-reactive protein (CRP).</p><p><strong>Conclusions: </strong>Wide resection and endoprosthetic reconstruction offer a reliable solution in selected patients with skeletal metastases. Higher age, fast-growing metastases (from bladder cancer, colorectal, hepatocellular, lung cancer, malignant melanoma, unknown origin), pathologic fracture or >1 metastasis and elevated CRP predict shorter patient survival and may represent a relative contraindication in this regard.</p>\",\"PeriodicalId\":21034,\"journal\":{\"name\":\"Radiology and Oncology\",\"volume\":\" \",\"pages\":\"450-456\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-03-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12441881/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiology and Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2478/raon-2025-0009\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiology and Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2478/raon-2025-0009","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:这项2009-2021年全国队列研究的目的是分析阑尾骨转移切除患者和假体重建的术后生存率,并与肉瘤患者和非肿瘤性重建患者进行比较。患者和方法:根据2013-SPRING预测模型,将144例连续肿瘤内假体重建患者(32例转移性切除患者,73例肉瘤患者,39例非肿瘤性患者)分为组织病理学组。采用Kaplan-Meier法和Cox回归分析生存率。结果:快速/中等/缓慢生长转移瘤广泛切除后2年生存率为25/55/88%,5年生存率为10/30/83%,而肉瘤2年生存率为80%,5年生存率为69%。与肉瘤相比,骨转移瘤切除后的估计平均术后生存期明显缩短(4.6年对9.1年,log-rank p < 0.001)。患者生存差的预测因素包括年龄增大、病理性骨折或bbb1转移、诊断组快速转移和术前c反应蛋白(CRP)升高。结论:广泛切除和假体内重建是治疗骨转移瘤的可靠方法。年龄增大、快速转移(膀胱癌、结直肠癌、肝细胞癌、肺癌、恶性黑色素瘤、来源不明)、病理性骨折或bbb1转移和CRP升高预示患者生存期较短,这可能是这方面的相对禁忌症。
Patient survival after resection of skeletal metastases and endoprosthetic reconstruction: a nation-wide cohort study in a single oncological institution.
Background: The aim of this nation-wide 2009-2021 cohort study was to analyze postoperative survival of patients with resected appendicular skeletal metastases and endoprosthetic reconstruction in comparison to sarcoma patients and non-oncological reconstructions.
Patients and methods: A single institution nation-wide cohort of 144 consecutive patients with tumor endoprosthetic reconstructions (32 resected metastases, 73 resected sarcomas, 39 non-oncological) were stratified into histopathological groups according to the 2013-SPRING prediction model. Their survival was analyzed with the Kaplan-Meier method and Cox regression.
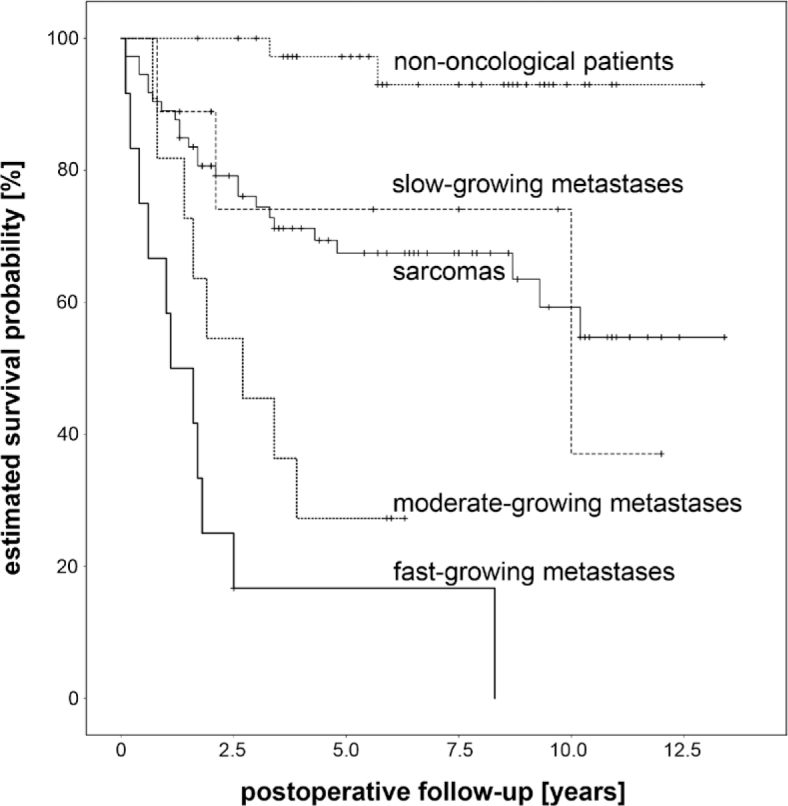
Results: The observed patient survival rates after wide resection of fast/moderate/slow growing metastases were 25/55/88% at 2 years and 10/30/83% at 5 years, while in sarcomas the observed survival rates were 80% at 2 years and 69% at 5 years. Estimated mean postoperative survival after resection of skeletal metastases was significantly shorter in comparison to sarcomas (4.6 years vs. 9.1 years, log-rank p < 0.001). Predictors of worse patient survival included higher age, pathologic fracture or >1 metastasis, diagnostic group fast-growing metastases and higher preoperative C-reactive protein (CRP).
Conclusions: Wide resection and endoprosthetic reconstruction offer a reliable solution in selected patients with skeletal metastases. Higher age, fast-growing metastases (from bladder cancer, colorectal, hepatocellular, lung cancer, malignant melanoma, unknown origin), pathologic fracture or >1 metastasis and elevated CRP predict shorter patient survival and may represent a relative contraindication in this regard.
期刊介绍:
Radiology and Oncology is a multidisciplinary journal devoted to the publishing original and high quality scientific papers and review articles, pertinent to diagnostic and interventional radiology, computerized tomography, magnetic resonance, ultrasound, nuclear medicine, radiotherapy, clinical and experimental oncology, radiobiology, medical physics and radiation protection. Therefore, the scope of the journal is to cover beside radiology the diagnostic and therapeutic aspects in oncology, which distinguishes it from other journals in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


