G Lemvik, L Larsson, F Rudolf, J E Vejrum, M Sodemann, V F Gomes, C Wejse
{"title":"一项关于儿童结核病预防治疗的开放标签集群随机试验。","authors":"G Lemvik, L Larsson, F Rudolf, J E Vejrum, M Sodemann, V F Gomes, C Wejse","doi":"10.5588/ijtldopen.24.0467","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In a study on 9 months of isoniazid preventive therapy (IPT) in children in Guinea-Bissau, 76% of children exposed to TB at home completed 6 months of IPT. We aimed to test whether 4 months of rifampicin and isoniazid (RH) would improve adherence compared to 9 months of isoniazid (INH).</p><p><strong>Methods: </strong>We conducted an open-label cluster-randomised superiority study in children aged <15 years living with a TB case. Children were randomised by house to receive 4 months of RH or 9 months of INH. RH was given as a fixed-combination pill. The primary outcome was adherence, defined as taking >80% of prescribed dosages per month, assessed by pill count. Our aim was 3 months of RH or 6 months of INH.</p><p><strong>Results: </strong>A total of 752 children from 223 houses were included, 354 in the INH group and 398 in the RH group. Overall, 57% of the children took >80% of the prescribed pills. In the INH group, 68% completed 6 months of therapy, while 61% of the RH group completed 3 months (OR 1.32, 95% CI 0.90-1.95). The main reason for non-adherence in both groups was travel or relocation, accounting for 50% of missed doses.</p><p><strong>Conclusion: </strong>The shorter preventive therapy of 4 months of RH did not improve adherence in children in Guinea-Bissau. Travelling was the primary reason for non-adherence.</p>","PeriodicalId":519984,"journal":{"name":"IJTLD open","volume":"2 3","pages":"120-128"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11906030/pdf/","citationCount":"0","resultStr":"{\"title\":\"An open-label cluster-randomised trial on TB preventive therapy for children.\",\"authors\":\"G Lemvik, L Larsson, F Rudolf, J E Vejrum, M Sodemann, V F Gomes, C Wejse\",\"doi\":\"10.5588/ijtldopen.24.0467\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In a study on 9 months of isoniazid preventive therapy (IPT) in children in Guinea-Bissau, 76% of children exposed to TB at home completed 6 months of IPT. We aimed to test whether 4 months of rifampicin and isoniazid (RH) would improve adherence compared to 9 months of isoniazid (INH).</p><p><strong>Methods: </strong>We conducted an open-label cluster-randomised superiority study in children aged <15 years living with a TB case. Children were randomised by house to receive 4 months of RH or 9 months of INH. RH was given as a fixed-combination pill. The primary outcome was adherence, defined as taking >80% of prescribed dosages per month, assessed by pill count. Our aim was 3 months of RH or 6 months of INH.</p><p><strong>Results: </strong>A total of 752 children from 223 houses were included, 354 in the INH group and 398 in the RH group. Overall, 57% of the children took >80% of the prescribed pills. In the INH group, 68% completed 6 months of therapy, while 61% of the RH group completed 3 months (OR 1.32, 95% CI 0.90-1.95). The main reason for non-adherence in both groups was travel or relocation, accounting for 50% of missed doses.</p><p><strong>Conclusion: </strong>The shorter preventive therapy of 4 months of RH did not improve adherence in children in Guinea-Bissau. Travelling was the primary reason for non-adherence.</p>\",\"PeriodicalId\":519984,\"journal\":{\"name\":\"IJTLD open\",\"volume\":\"2 3\",\"pages\":\"120-128\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11906030/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"IJTLD open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5588/ijtldopen.24.0467\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJTLD open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5588/ijtldopen.24.0467","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
An open-label cluster-randomised trial on TB preventive therapy for children.
Background: In a study on 9 months of isoniazid preventive therapy (IPT) in children in Guinea-Bissau, 76% of children exposed to TB at home completed 6 months of IPT. We aimed to test whether 4 months of rifampicin and isoniazid (RH) would improve adherence compared to 9 months of isoniazid (INH).
Methods: We conducted an open-label cluster-randomised superiority study in children aged <15 years living with a TB case. Children were randomised by house to receive 4 months of RH or 9 months of INH. RH was given as a fixed-combination pill. The primary outcome was adherence, defined as taking >80% of prescribed dosages per month, assessed by pill count. Our aim was 3 months of RH or 6 months of INH.
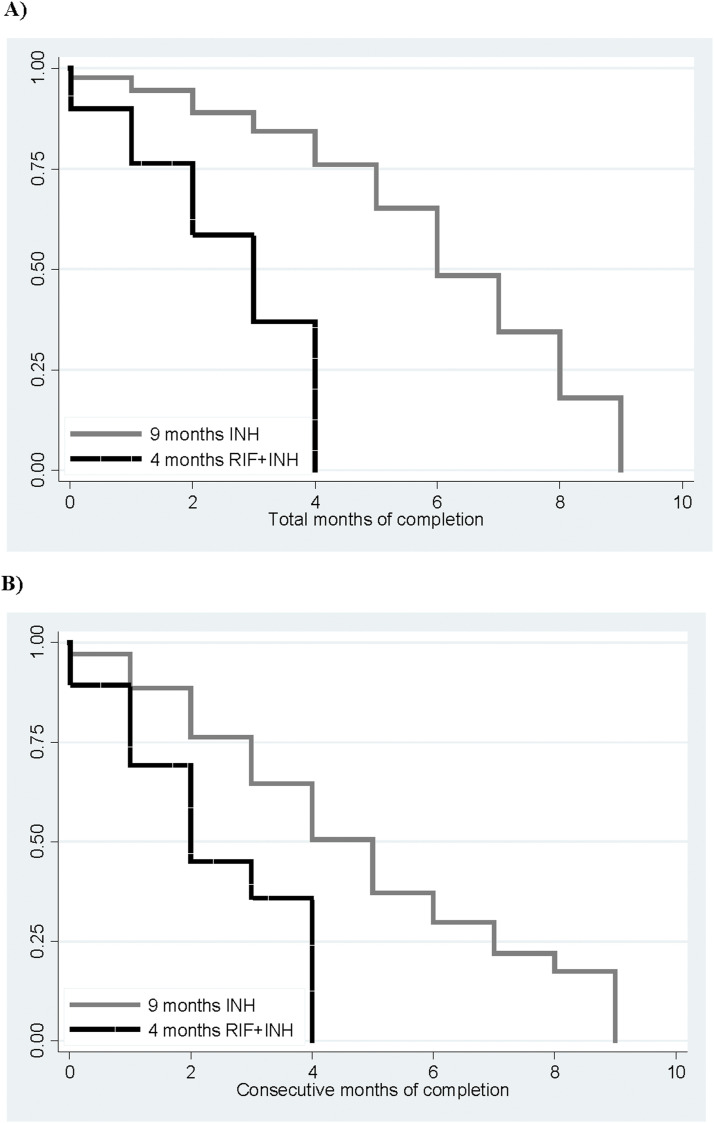
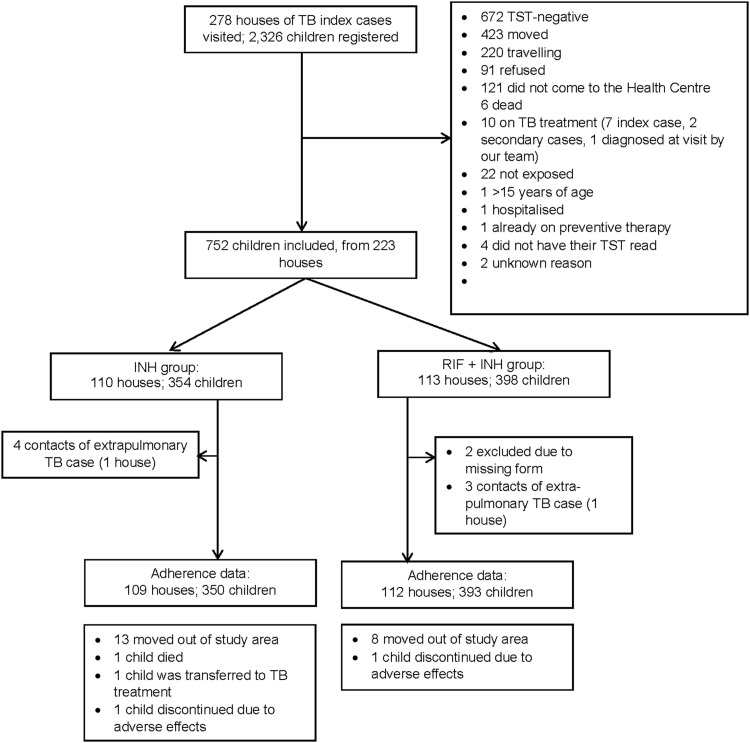
Results: A total of 752 children from 223 houses were included, 354 in the INH group and 398 in the RH group. Overall, 57% of the children took >80% of the prescribed pills. In the INH group, 68% completed 6 months of therapy, while 61% of the RH group completed 3 months (OR 1.32, 95% CI 0.90-1.95). The main reason for non-adherence in both groups was travel or relocation, accounting for 50% of missed doses.
Conclusion: The shorter preventive therapy of 4 months of RH did not improve adherence in children in Guinea-Bissau. Travelling was the primary reason for non-adherence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


