Areefa Alladin-Karan, Susan M Samuel, Andrew W Wade, Pietro Ravani, Silviu Grisaru, Ngan N Lam, Kathryn A Bernie, Robert R Quinn
{"title":"儿童IgA肾病与成人IgA肾病不同吗?叙述性评论。","authors":"Areefa Alladin-Karan, Susan M Samuel, Andrew W Wade, Pietro Ravani, Silviu Grisaru, Ngan N Lam, Kathryn A Bernie, Robert R Quinn","doi":"10.1177/20543581251322571","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of the review: </strong>Immunoglobulin A (IgA) nephropathy (IgAN) is the most common primary glomerular kidney disease. Children and adults are presumed to have the same disease and are treated similarly. However, there are differences between childhood IgAN and adult IgAN that may require unique treatment considerations, even after transition to adult nephrology services. A narrative review was conducted to compare childhood and adult IgAN and to describe the distinct characteristics of childhood IgAN. Reframing childhood IgAN can inform guideline recommendations unique to childhood IgAN, the development of targeted therapies, and clinical trial design.</p><p><strong>Sources of information: </strong>Medline and Embase were searched for reports on children and adults with IgAN published between January 2013 and December 2023 (updated May 2024). The search was not restricted by age group, outcomes reported, language, or study design. Randomized controlled trials (RCTs), observational studies, review articles, and nephrology conference abstracts were included. A total of 3104 reports were retrieved. Forty-seven reports (37 primary studies and 10 reviews) were included in the review. Two RCTs and 35 observational studies included a total of 45 085 participants (9223 children and 35 862 adults).</p><p><strong>Method: </strong>Data were extracted for primary IgAN and not for IgA vasculitis-associated nephritis. Findings were described with no statistical comparisons due to variations in interventions and outcome definitions.</p><p><strong>Key findings: </strong>Gross hematuria was the obvious clinical difference between childhood IgAN and adult (60-88% vs 15-20%). Nephrotic syndrome was more common in children, approaching up to 44%, while <18% of adults had nephrotic syndrome. Children were biopsied sooner (6 vs 15 months) and had more inflammatory kidney lesions (mesangial hypercellularity: 41-82% vs 38-64%; endocapillary hypercellularity: 39-58% vs 17-34%). Chronic kidney lesions were more prevalent in adults (segmental sclerosis: 62-77% vs 8-51%; interstitial fibrosis/tubular atrophy: 34-37% vs 1-18%). The use of immunosuppressive therapy was higher in children (46-84% vs 35-56%). Children were started on immunosuppressive therapy sooner than adults. Adults were more likely to be optimized with renin-angiotensin system inhibitors (87-94% vs 49-75%). Children had better kidney function than adults at diagnosis (estimated glomerular filtration rate of 90-128 vs 50-88 ml/min/1.73 m<sup>2</sup>), and children also had better kidney survival, with kidney failure of 3.1% vs 13.4% at 5 years. Children had more risk alleles for IgAN and higher levels of mannose-binding lectin than adults.</p><p><strong>Limitations: </strong>Most studies were retrospective and observational, with limited data on children and disease mechanisms. Data were not pooled for analysis because of important differences in definitions and measurements of baseline characteristics and outcomes. Data from countries with established urine screening programs were different compared to countries without urine screening programs. Some observed differences may be due to practice variation and delayed diagnosis in adults (lead-time bias). Well-designed prospective studies and standardized measures for kidney function assessment and outcomes can reduce heterogeneity and improve results from reviews.</p><p><strong>Conclusion: </strong>Inherent differences between childhood IgAN and adult IgAN may be due to distinct disease mechanisms. Approaching childhood IgAN as a separate condition could lead to the discovery of targeted therapies and improve management during childhood and after the transition to adult care.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251322571"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11898040/pdf/","citationCount":"0","resultStr":"{\"title\":\"Is Childhood IgA Nephropathy Different From Adult IgA Nephropathy? A Narrative Review.\",\"authors\":\"Areefa Alladin-Karan, Susan M Samuel, Andrew W Wade, Pietro Ravani, Silviu Grisaru, Ngan N Lam, Kathryn A Bernie, Robert R Quinn\",\"doi\":\"10.1177/20543581251322571\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose of the review: </strong>Immunoglobulin A (IgA) nephropathy (IgAN) is the most common primary glomerular kidney disease. Children and adults are presumed to have the same disease and are treated similarly. However, there are differences between childhood IgAN and adult IgAN that may require unique treatment considerations, even after transition to adult nephrology services. A narrative review was conducted to compare childhood and adult IgAN and to describe the distinct characteristics of childhood IgAN. Reframing childhood IgAN can inform guideline recommendations unique to childhood IgAN, the development of targeted therapies, and clinical trial design.</p><p><strong>Sources of information: </strong>Medline and Embase were searched for reports on children and adults with IgAN published between January 2013 and December 2023 (updated May 2024). The search was not restricted by age group, outcomes reported, language, or study design. Randomized controlled trials (RCTs), observational studies, review articles, and nephrology conference abstracts were included. A total of 3104 reports were retrieved. Forty-seven reports (37 primary studies and 10 reviews) were included in the review. Two RCTs and 35 observational studies included a total of 45 085 participants (9223 children and 35 862 adults).</p><p><strong>Method: </strong>Data were extracted for primary IgAN and not for IgA vasculitis-associated nephritis. Findings were described with no statistical comparisons due to variations in interventions and outcome definitions.</p><p><strong>Key findings: </strong>Gross hematuria was the obvious clinical difference between childhood IgAN and adult (60-88% vs 15-20%). Nephrotic syndrome was more common in children, approaching up to 44%, while <18% of adults had nephrotic syndrome. Children were biopsied sooner (6 vs 15 months) and had more inflammatory kidney lesions (mesangial hypercellularity: 41-82% vs 38-64%; endocapillary hypercellularity: 39-58% vs 17-34%). Chronic kidney lesions were more prevalent in adults (segmental sclerosis: 62-77% vs 8-51%; interstitial fibrosis/tubular atrophy: 34-37% vs 1-18%). The use of immunosuppressive therapy was higher in children (46-84% vs 35-56%). Children were started on immunosuppressive therapy sooner than adults. Adults were more likely to be optimized with renin-angiotensin system inhibitors (87-94% vs 49-75%). Children had better kidney function than adults at diagnosis (estimated glomerular filtration rate of 90-128 vs 50-88 ml/min/1.73 m<sup>2</sup>), and children also had better kidney survival, with kidney failure of 3.1% vs 13.4% at 5 years. Children had more risk alleles for IgAN and higher levels of mannose-binding lectin than adults.</p><p><strong>Limitations: </strong>Most studies were retrospective and observational, with limited data on children and disease mechanisms. Data were not pooled for analysis because of important differences in definitions and measurements of baseline characteristics and outcomes. Data from countries with established urine screening programs were different compared to countries without urine screening programs. Some observed differences may be due to practice variation and delayed diagnosis in adults (lead-time bias). Well-designed prospective studies and standardized measures for kidney function assessment and outcomes can reduce heterogeneity and improve results from reviews.</p><p><strong>Conclusion: </strong>Inherent differences between childhood IgAN and adult IgAN may be due to distinct disease mechanisms. Approaching childhood IgAN as a separate condition could lead to the discovery of targeted therapies and improve management during childhood and after the transition to adult care.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"12 \",\"pages\":\"20543581251322571\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-03-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11898040/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581251322571\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251322571","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
免疫球蛋白A (IgA)肾病(IgAN)是最常见的原发性肾小球肾病。儿童和成人被认为患有同样的疾病,并得到同样的治疗。然而,儿童IgAN和成人IgAN之间存在差异,可能需要独特的治疗考虑,即使在过渡到成人肾病服务之后。对儿童期和成年期IgAN进行了回顾性比较,并描述了儿童期IgAN的不同特征。重新构建儿童IgAN可以为儿童IgAN的独特指南建议、靶向治疗的发展和临床试验设计提供信息。信息来源:在Medline和Embase检索2013年1月至2023年12月(更新于2024年5月)发表的关于儿童和成人IgAN的报告。搜索不受年龄组、结果报告、语言或研究设计的限制。随机对照试验(RCTs)、观察性研究、综述文章和肾脏病会议摘要被纳入。总共检索了3104份报告。47份报告(37项初步研究和10项综述)被纳入本综述。两项随机对照试验和35项观察性研究共纳入45 085名参与者(9223名儿童和35 862名成人)。方法:提取原发性IgAN的数据,而不提取IgA血管炎相关性肾炎的数据。由于干预措施和结果定义的差异,研究结果没有进行统计比较。主要发现:肉眼血尿是儿童IgAN与成人的明显临床差异(60-88% vs 15-20%)。肾病综合征在儿童中更常见,接近44%,而2),儿童也有更好的肾脏存活率,5年肾衰竭为3.1%比13.4%。与成人相比,儿童有更多的IgAN风险等位基因和更高水平的甘露糖结合凝集素。局限性:大多数研究是回顾性和观察性的,关于儿童和疾病机制的数据有限。由于基线特征和结果的定义和测量存在重要差异,因此没有将数据汇总进行分析。已建立尿液筛查项目的国家与未建立尿液筛查项目的国家的数据有所不同。一些观察到的差异可能是由于实践差异和成人的延迟诊断(前置时间偏差)。设计良好的前瞻性研究和标准化的肾功能评估和结果测量方法可以减少异质性并改善综述的结果。结论:儿童IgAN与成人IgAN的内在差异可能是由于不同的疾病机制。将儿童IgAN作为一种单独的疾病来对待,可能会导致发现有针对性的治疗方法,并改善儿童时期和过渡到成人护理后的管理。
Is Childhood IgA Nephropathy Different From Adult IgA Nephropathy? A Narrative Review.
Purpose of the review: Immunoglobulin A (IgA) nephropathy (IgAN) is the most common primary glomerular kidney disease. Children and adults are presumed to have the same disease and are treated similarly. However, there are differences between childhood IgAN and adult IgAN that may require unique treatment considerations, even after transition to adult nephrology services. A narrative review was conducted to compare childhood and adult IgAN and to describe the distinct characteristics of childhood IgAN. Reframing childhood IgAN can inform guideline recommendations unique to childhood IgAN, the development of targeted therapies, and clinical trial design.
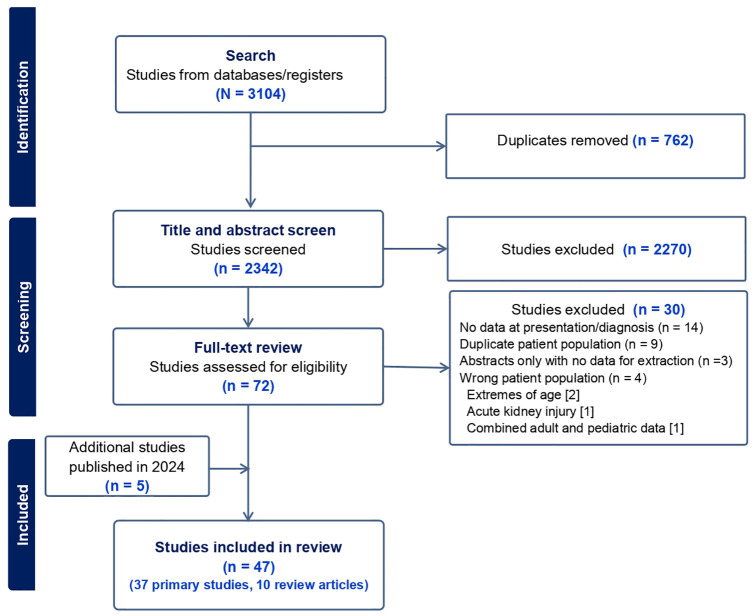
Sources of information: Medline and Embase were searched for reports on children and adults with IgAN published between January 2013 and December 2023 (updated May 2024). The search was not restricted by age group, outcomes reported, language, or study design. Randomized controlled trials (RCTs), observational studies, review articles, and nephrology conference abstracts were included. A total of 3104 reports were retrieved. Forty-seven reports (37 primary studies and 10 reviews) were included in the review. Two RCTs and 35 observational studies included a total of 45 085 participants (9223 children and 35 862 adults).
Method: Data were extracted for primary IgAN and not for IgA vasculitis-associated nephritis. Findings were described with no statistical comparisons due to variations in interventions and outcome definitions.
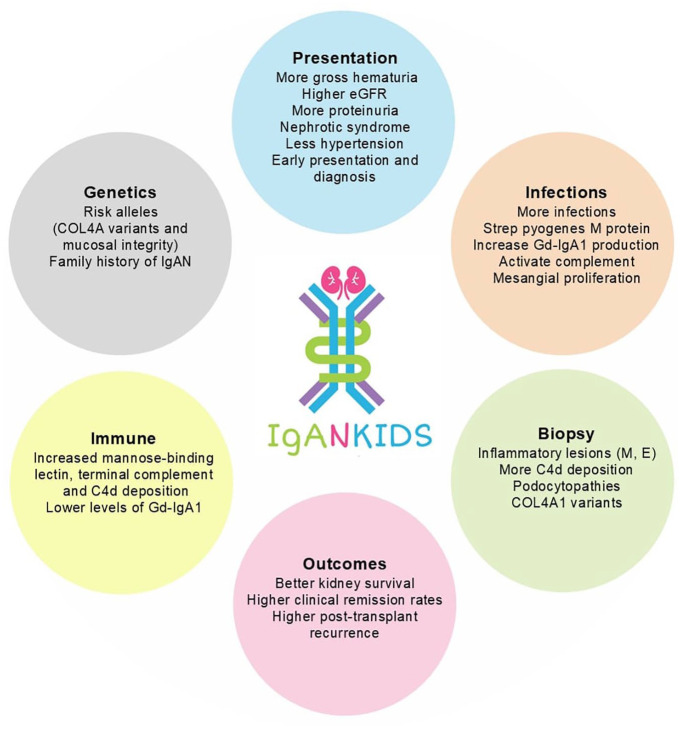
Key findings: Gross hematuria was the obvious clinical difference between childhood IgAN and adult (60-88% vs 15-20%). Nephrotic syndrome was more common in children, approaching up to 44%, while <18% of adults had nephrotic syndrome. Children were biopsied sooner (6 vs 15 months) and had more inflammatory kidney lesions (mesangial hypercellularity: 41-82% vs 38-64%; endocapillary hypercellularity: 39-58% vs 17-34%). Chronic kidney lesions were more prevalent in adults (segmental sclerosis: 62-77% vs 8-51%; interstitial fibrosis/tubular atrophy: 34-37% vs 1-18%). The use of immunosuppressive therapy was higher in children (46-84% vs 35-56%). Children were started on immunosuppressive therapy sooner than adults. Adults were more likely to be optimized with renin-angiotensin system inhibitors (87-94% vs 49-75%). Children had better kidney function than adults at diagnosis (estimated glomerular filtration rate of 90-128 vs 50-88 ml/min/1.73 m2), and children also had better kidney survival, with kidney failure of 3.1% vs 13.4% at 5 years. Children had more risk alleles for IgAN and higher levels of mannose-binding lectin than adults.
Limitations: Most studies were retrospective and observational, with limited data on children and disease mechanisms. Data were not pooled for analysis because of important differences in definitions and measurements of baseline characteristics and outcomes. Data from countries with established urine screening programs were different compared to countries without urine screening programs. Some observed differences may be due to practice variation and delayed diagnosis in adults (lead-time bias). Well-designed prospective studies and standardized measures for kidney function assessment and outcomes can reduce heterogeneity and improve results from reviews.
Conclusion: Inherent differences between childhood IgAN and adult IgAN may be due to distinct disease mechanisms. Approaching childhood IgAN as a separate condition could lead to the discovery of targeted therapies and improve management during childhood and after the transition to adult care.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


