{"title":"胸升主动脉瘤的4D血流磁共振成像及流固耦合分析。","authors":"Yu Zhu, Chlöe Armour, Binghuan Li, Selene Pirola, Yousuf Salmasi, Thanos Athanasiou, Declan P. O’Regan, Xiao Yun Xu","doi":"10.1007/s10237-025-01939-6","DOIUrl":null,"url":null,"abstract":"<div><p>This study aimed to characterize the altered hemodynamics and wall mechanics in ascending thoracic aortic aneurysms (ATAA) by employing fully coupled two-way fluid–structure interaction (FSI) analyses. Our FSI models incorporated hyperelastic wall mechanical properties, prestress, and patient-specific inlet velocity profiles (IVP) extracted from 4D flow magnetic resonance imaging (MRI). By performing FSI analyses on 7 patient-specific ATAA models and 6 healthy aortas, the primary objective of the study was to compare hemodynamic and biomechanical features in ATAA versus healthy controls. A secondary objective was to examine the need for 4D flow MRI-derived IVP in FSI simulations by comparing results with those using two commonly adopted idealized IVPs: Flat-IVP and Para-IVP for selected cases. Our results show that, compared to the healthy aortas, the ATAA models exhibited highly disturbed blood flow in the ascending aorta. Consequently, maximum turbulent kinetic energy (TKE) at peak systole (155.0 ± 188.4 Pa) and maximum time-averaged wall shear stress (TAWSS) (8.6 ± 6.5 Pa) were significantly higher in the ATAA cohort, compared to 0.6 ± 0.5 Pa and 2.8 ± 0.7 Pa in the healthy aortas. Peak wall stress was also nearly doubled in the ATAA group (414 ± 108 kPa vs. 215 ± 31 kPa). Additionally, comparisons of simulation results across models with different IVPs underscore the importance of prescribing 3D-IVP at the inlet, especially for ATAA cases. Using idealized IVPs in two selected ATAA models (P1 and P7) substantially reduced the maximum TKE from 571 Pa to 0.01 Pa (Flat-IVP) and 0.02 Pa (Para-IVP) in P1 and from 73 Pa to 0.01 Pa (Flat-IVP) and 0.08 Pa (Para-IVP) in P7, while the maximum TAWSS in the ascending aorta decreased from 9.6 Pa to 0.7 Pa (Flat-IVP) and 0.9 Pa (Para-IVP) in P1, and from 3.6 Pa to 1.2 Pa and 0.9 Pa, respectively, in P7. Moreover, idealized IVPs also caused the peak wall stress to reduce by up to 11.5% in P1 with severe aortic valve stenosis, and by up to 2% in P7 with mild aortic regurgitation. These results highlight the importance of FSI simulations combined with 4D flow MRI in capturing realistic hemodynamic and biomechanical changes in aneurysmal aortas.</p></div>","PeriodicalId":489,"journal":{"name":"Biomechanics and Modeling in Mechanobiology","volume":"24 3","pages":"829 - 844"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12162810/pdf/","citationCount":"0","resultStr":"{\"title\":\"A combined 4D flow MR imaging and fluid–structure interaction analysis of ascending thoracic aortic aneurysms\",\"authors\":\"Yu Zhu, Chlöe Armour, Binghuan Li, Selene Pirola, Yousuf Salmasi, Thanos Athanasiou, Declan P. O’Regan, Xiao Yun Xu\",\"doi\":\"10.1007/s10237-025-01939-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>This study aimed to characterize the altered hemodynamics and wall mechanics in ascending thoracic aortic aneurysms (ATAA) by employing fully coupled two-way fluid–structure interaction (FSI) analyses. Our FSI models incorporated hyperelastic wall mechanical properties, prestress, and patient-specific inlet velocity profiles (IVP) extracted from 4D flow magnetic resonance imaging (MRI). By performing FSI analyses on 7 patient-specific ATAA models and 6 healthy aortas, the primary objective of the study was to compare hemodynamic and biomechanical features in ATAA versus healthy controls. A secondary objective was to examine the need for 4D flow MRI-derived IVP in FSI simulations by comparing results with those using two commonly adopted idealized IVPs: Flat-IVP and Para-IVP for selected cases. Our results show that, compared to the healthy aortas, the ATAA models exhibited highly disturbed blood flow in the ascending aorta. Consequently, maximum turbulent kinetic energy (TKE) at peak systole (155.0 ± 188.4 Pa) and maximum time-averaged wall shear stress (TAWSS) (8.6 ± 6.5 Pa) were significantly higher in the ATAA cohort, compared to 0.6 ± 0.5 Pa and 2.8 ± 0.7 Pa in the healthy aortas. Peak wall stress was also nearly doubled in the ATAA group (414 ± 108 kPa vs. 215 ± 31 kPa). Additionally, comparisons of simulation results across models with different IVPs underscore the importance of prescribing 3D-IVP at the inlet, especially for ATAA cases. Using idealized IVPs in two selected ATAA models (P1 and P7) substantially reduced the maximum TKE from 571 Pa to 0.01 Pa (Flat-IVP) and 0.02 Pa (Para-IVP) in P1 and from 73 Pa to 0.01 Pa (Flat-IVP) and 0.08 Pa (Para-IVP) in P7, while the maximum TAWSS in the ascending aorta decreased from 9.6 Pa to 0.7 Pa (Flat-IVP) and 0.9 Pa (Para-IVP) in P1, and from 3.6 Pa to 1.2 Pa and 0.9 Pa, respectively, in P7. Moreover, idealized IVPs also caused the peak wall stress to reduce by up to 11.5% in P1 with severe aortic valve stenosis, and by up to 2% in P7 with mild aortic regurgitation. These results highlight the importance of FSI simulations combined with 4D flow MRI in capturing realistic hemodynamic and biomechanical changes in aneurysmal aortas.</p></div>\",\"PeriodicalId\":489,\"journal\":{\"name\":\"Biomechanics and Modeling in Mechanobiology\",\"volume\":\"24 3\",\"pages\":\"829 - 844\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-03-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12162810/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biomechanics and Modeling in Mechanobiology\",\"FirstCategoryId\":\"5\",\"ListUrlMain\":\"https://link.springer.com/article/10.1007/s10237-025-01939-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"BIOPHYSICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomechanics and Modeling in Mechanobiology","FirstCategoryId":"5","ListUrlMain":"https://link.springer.com/article/10.1007/s10237-025-01939-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"BIOPHYSICS","Score":null,"Total":0}
引用次数: 0
摘要
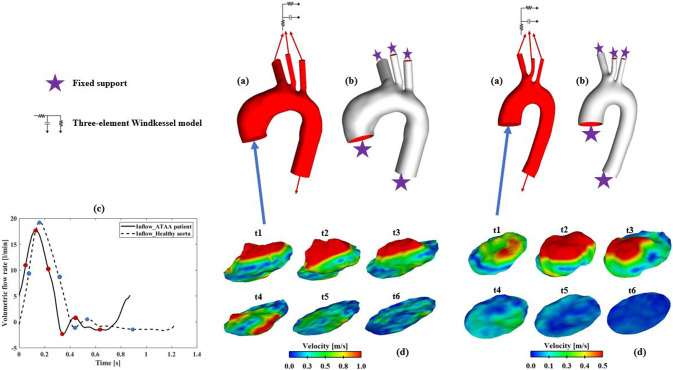
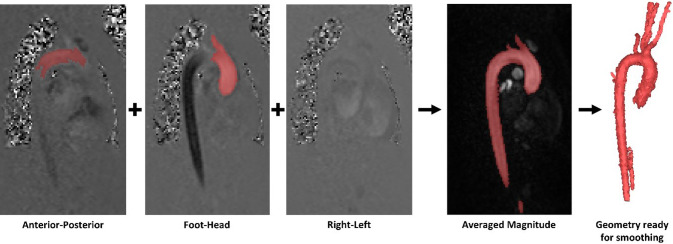
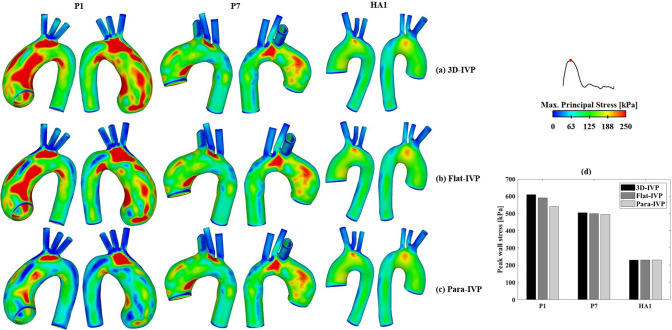
本研究旨在通过完全耦合的双向流固相互作用(FSI)分析来表征升胸主动脉瘤(ATAA)血流动力学和壁力学的改变。我们的FSI模型结合了超弹性壁力学特性、预应力和从4D流动磁共振成像(MRI)中提取的患者特定入口速度剖面(IVP)。通过对7例患者特异性ATAA模型和6条健康主动脉进行FSI分析,研究的主要目的是比较ATAA与健康对照组的血流动力学和生物力学特征。第二个目标是通过比较两种常用的理想IVP (Flat-IVP和Para-IVP)的结果,检查在FSI模拟中需用4D血流mri衍生的IVP。我们的研究结果表明,与健康主动脉相比,ATAA模型的升主动脉血流受到高度干扰。因此,与健康主动脉的0.6±0.5 Pa和2.8±0.7 Pa相比,ATAA组收缩峰值时的最大湍流动能(TKE)(155.0±188.4 Pa)和最大时间平均壁剪切应力(TAWSS)(8.6±6.5 Pa)显著更高。ATAA组的峰值壁应力也增加了近一倍(414±108 kPa vs 215±31 kPa)。此外,对不同ivp模型的模拟结果进行比较,强调了在进气道开具3D-IVP处方的重要性,特别是对于ATAA病例。在两个选定的ATAA模型(P1和P7)中使用理想的IVPs,可使P1的最大TKE从571 Pa降至0.01 Pa (Flat-IVP)和0.02 Pa (Para-IVP), P7的最大TKE从73 Pa降至0.01 Pa (Flat-IVP)和0.08 Pa (Para-IVP),而升主动脉的最大TAWSS从P1的9.6 Pa降至0.7 Pa (Flat-IVP)和0.9 Pa (Para-IVP), P7的最大TAWSS分别从3.6 Pa降至1.2 Pa和0.9 Pa。此外,理想的IVPs还使严重主动脉瓣狭窄的P1患者的峰值壁应力降低了11.5%,轻度主动脉瓣反流的P7患者的峰值壁应力降低了2%。这些结果强调了FSI模拟结合4D血流MRI在捕捉动脉瘤主动脉真实血流动力学和生物力学变化方面的重要性。
A combined 4D flow MR imaging and fluid–structure interaction analysis of ascending thoracic aortic aneurysms
This study aimed to characterize the altered hemodynamics and wall mechanics in ascending thoracic aortic aneurysms (ATAA) by employing fully coupled two-way fluid–structure interaction (FSI) analyses. Our FSI models incorporated hyperelastic wall mechanical properties, prestress, and patient-specific inlet velocity profiles (IVP) extracted from 4D flow magnetic resonance imaging (MRI). By performing FSI analyses on 7 patient-specific ATAA models and 6 healthy aortas, the primary objective of the study was to compare hemodynamic and biomechanical features in ATAA versus healthy controls. A secondary objective was to examine the need for 4D flow MRI-derived IVP in FSI simulations by comparing results with those using two commonly adopted idealized IVPs: Flat-IVP and Para-IVP for selected cases. Our results show that, compared to the healthy aortas, the ATAA models exhibited highly disturbed blood flow in the ascending aorta. Consequently, maximum turbulent kinetic energy (TKE) at peak systole (155.0 ± 188.4 Pa) and maximum time-averaged wall shear stress (TAWSS) (8.6 ± 6.5 Pa) were significantly higher in the ATAA cohort, compared to 0.6 ± 0.5 Pa and 2.8 ± 0.7 Pa in the healthy aortas. Peak wall stress was also nearly doubled in the ATAA group (414 ± 108 kPa vs. 215 ± 31 kPa). Additionally, comparisons of simulation results across models with different IVPs underscore the importance of prescribing 3D-IVP at the inlet, especially for ATAA cases. Using idealized IVPs in two selected ATAA models (P1 and P7) substantially reduced the maximum TKE from 571 Pa to 0.01 Pa (Flat-IVP) and 0.02 Pa (Para-IVP) in P1 and from 73 Pa to 0.01 Pa (Flat-IVP) and 0.08 Pa (Para-IVP) in P7, while the maximum TAWSS in the ascending aorta decreased from 9.6 Pa to 0.7 Pa (Flat-IVP) and 0.9 Pa (Para-IVP) in P1, and from 3.6 Pa to 1.2 Pa and 0.9 Pa, respectively, in P7. Moreover, idealized IVPs also caused the peak wall stress to reduce by up to 11.5% in P1 with severe aortic valve stenosis, and by up to 2% in P7 with mild aortic regurgitation. These results highlight the importance of FSI simulations combined with 4D flow MRI in capturing realistic hemodynamic and biomechanical changes in aneurysmal aortas.
期刊介绍:
Mechanics regulates biological processes at the molecular, cellular, tissue, organ, and organism levels. A goal of this journal is to promote basic and applied research that integrates the expanding knowledge-bases in the allied fields of biomechanics and mechanobiology. Approaches may be experimental, theoretical, or computational; they may address phenomena at the nano, micro, or macrolevels. Of particular interest are investigations that
(1) quantify the mechanical environment in which cells and matrix function in health, disease, or injury,
(2) identify and quantify mechanosensitive responses and their mechanisms,
(3) detail inter-relations between mechanics and biological processes such as growth, remodeling, adaptation, and repair, and
(4) report discoveries that advance therapeutic and diagnostic procedures.
Especially encouraged are analytical and computational models based on solid mechanics, fluid mechanics, or thermomechanics, and their interactions; also encouraged are reports of new experimental methods that expand measurement capabilities and new mathematical methods that facilitate analysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


