Maria Teresa Bilotta, Paola Vacca, Mariacristina Esposito, Luca Buzzonetti, Giuseppe Bianco, Alessandro Giovanni Fiocchi, Lorenzo Moretta, Massimiliano Raponi, Maria Cristina Artesani, Nicola Tumino
{"title":"春性角膜结膜炎的免疫分型:用于治疗反应预测的Schirmer试验。","authors":"Maria Teresa Bilotta, Paola Vacca, Mariacristina Esposito, Luca Buzzonetti, Giuseppe Bianco, Alessandro Giovanni Fiocchi, Lorenzo Moretta, Massimiliano Raponi, Maria Cristina Artesani, Nicola Tumino","doi":"10.1111/all.16525","DOIUrl":null,"url":null,"abstract":"<p>Vernal keratoconjunctivitis (VKC) is a disease of the anterior segment of the eye primarily affecting children. Diagnosis is confirmed by the evidence of signs such as an upper tarsal papillary reaction or limbal conjunctival nodules (Trantas dots) and is classified as tarsal (T) or limbal (L), respectively, or mixed (M) when both signs are present [<span>1-4</span>]. The symptoms of VKC have a seasonal pattern, although some patients develop a chronic form [<span>5</span>]. Topical antiallergic drugs may be effective for mild cases, while more severe cases require topical corticosteroids or immunosuppressant eye drops [<span>3, 6, 7</span>].</p><p>VKC may have a genetic substrate [<span>8, 9</span>], but recognizes in its pathophysiology an immunological involvement, with both IgE- and non-IgE-mediated mechanisms [<span>2, 10-12</span>].</p><p>Until now, the ocular cellular landscape has been characterized using different methods of tear collection (i.e., impression cytology, conjunctival brushing or biopsy, microcapillary or surgical sponge methods, aspiration techniques, or Schirmer test paper) [<span>13-16</span>].</p><p>We investigated the Schirmer test's potential uses to assess the conjunctival surface's immunological content. Among all the others, this test is the least bothersome and painful method of tear collection, especially in the pediatric population where it is routinely performed during the first-level ophthalmological evaluation in patients with VKC [<span>17</span>].</p><p>We studied 58 samples derived from VKC patients analyzed at diagnosis and/or during treatment, whose clinical and demographic characteristics are summarized in Table S1.</p><p>Cells collected from paper filters used in the Schirmer test (see Appendix S1) were enriched with leukocytes exhibiting low granularity (Figure 1A). We observed a significant increase in the absolute number, normalized by the size of the tears calculated with the Schirmer test itself, and percentages of leukocytes (CD45<sup>+</sup>cells) in inflamed ocular surfaces in untreated (group 1) compared with treated (group 2) VKC patients (Figure 1B). Among the treated patients (group 2), it was possible to identify, based on clinical characteristics (i.e., disappearance or attenuation of clinical symptoms) and by meta-analysis studies [<span>18</span>], a group of patients who did not respond (group 2-NR) and a group of patients who responded (group 2-R) to therapy. In particular, 2-NR patients displayed higher amounts and percentages of leukocytes than 2-R patients (Figure 1B). Highly activated leukocytes (% of CD45<sup>+</sup>HLA-DR<sup>+</sup>) were observed in group 1 compared to group 2 patients (Figure 1B). 2-NR patients showed a higher HLA-DR expression than 2-R patients, confirming the correlation between the activation status and the response to therapy (Figure 1B).</p><p>We specifically characterized the immune cell composition by analyzing specific markers to identify T-, B-, NK- cells, and monocytes (Figure 1C,D). Our data showed increased T-cell infiltration in untreated compared to treated VKC patients. Similarly, 2-NR patients displayed a higher frequency of T cells than 2-R patients (Figure 1E). No significant differences were observed regarding B cells, monocytes, and NK cells in all groups analyzed (Figure 1E).</p><p>In our cohort of pediatric VKC patients, we have defined different ranges to classify the pathological status and the response to therapy. Untreated patients presented more than 3000 CD45<sup>+</sup> cells infiltrated, treated 2-NR patients had more than 2000 CD45<sup>+</sup> cells, while 2-R patients did not exceed 300 CD45<sup>+</sup> cells (Figure 2A). Moreover, evaluating T cells can be a further marker to distinguish untreated and 2-NR versus 2-R patients (Figure 2B). Of note, the number of leukocytes directly correlates with the clinical classification (T, L, M) suggesting the importance of this tool for clinical purposes (Figure 2C).</p><p>The clinical applicability of the established ranges was further verified by analyzing leukocyte infiltration. Figure 2D shows two representative patients, examined at T1 after the end of the treatment with the first cycle of cyclosporine (CsA) and at T2, continuing or changing therapy. These two patients showed different responses to the CsA treatment at T1 (T1<sub>c</sub>); indeed, patient 1, who had at T1 high levels of leukocytes (Figure 2D, T1<sub>c</sub>), corresponding to the red area of Figure 2A (containing the two groups of patients 1 and 2-NR), displayed severe symptoms (Figure 2E, panels a-b). At T2, the symptoms were resolved (Figure 2E, panels c-d) with Tacrolimus-based eye drops treatment, with a consequent reduction of leukocyte infiltration (Figure 2D, T2<sub>t</sub>). Meanwhile, patient 2 at T1 had a leukocyte count (Figure 2D, T1<sub>c</sub> and 2E panels e-f) that fell within the green range in Figure 2A (corresponding to group 2-R), continued treatment with CsA, and at T2 achieved clinical resolution (Figure 2E, panels g-h), with a reduction in leukocyte numbers (Figure 2D, T2<sub>c</sub>). Similar results were observed when we evaluated the frequency of T cells (Figure S1).</p><p>Among patients treated with CsA, the ratio (> 1) of leukocytes (T2 vs. T1) highlighted that patients with the mixed form of the disease at T1 did not respond to the continuous CsA treatment (Figure 2F). These data could be helpful in suggesting a switching therapy from CsA to tacrolimus eye drops based on the evaluation of leukocyte number.</p><p>In conclusion, all these data suggest that the Schirmer test and clinical observation may be supportive in easily identifying an immune landscape useful for clinical purposes to classify VKC patients. Topical CsA and tacrolimus in allergic eye diseases are efficient in treating children and young patients affected by VKC [<span>7</span>]. However, previous literature indicates that the effectiveness of these topical treatments varies across different symptoms and signs, emphasizing the need for improved studies, consensus on core outcomes, and the potential for individualized therapy [<span>18</span>]. In this context, our study aims to characterize immune cells to enhance monitoring and establish a therapeutic regimen, or even discontinue therapy based on the number of leukocytes present.</p><p><b>Maria Teresa Bilotta:</b> methodology, formal analysis, investigation, data curation, writing – original draft, writing – review and editing. <b>Massimiliano Raponi:</b> writing-review and editing, formal analysis. <b>Mariacristina Esposito:</b> investigation, data curation. <b>Giuseppe Bianco:</b> methodology. <b>Luca Buzzonetti</b>, <b>Alessandro Giovanni Fiocchi</b>, and <b>Lorenzo Moretta:</b> writing – original draft, writing – review and editing, supervision. <b>Paola Vacca</b>, <b>Nicola Tumino</b>, and <b>Maria Cristina Artesani:</b> conceptualization, formal analysis, methodology, data curation, writing – original draft, writing – review and editing, supervision, funding acquisition, project administration, investigation.</p><p>The authors have nothing to report.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":122,"journal":{"name":"Allergy","volume":"80 7","pages":"2050-2054"},"PeriodicalIF":12.0000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/all.16525","citationCount":"0","resultStr":"{\"title\":\"Immunophenotyping in Vernal Keratoconjunctivitis: Schirmer Test for Therapy Response Prediction\",\"authors\":\"Maria Teresa Bilotta, Paola Vacca, Mariacristina Esposito, Luca Buzzonetti, Giuseppe Bianco, Alessandro Giovanni Fiocchi, Lorenzo Moretta, Massimiliano Raponi, Maria Cristina Artesani, Nicola Tumino\",\"doi\":\"10.1111/all.16525\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Vernal keratoconjunctivitis (VKC) is a disease of the anterior segment of the eye primarily affecting children. Diagnosis is confirmed by the evidence of signs such as an upper tarsal papillary reaction or limbal conjunctival nodules (Trantas dots) and is classified as tarsal (T) or limbal (L), respectively, or mixed (M) when both signs are present [<span>1-4</span>]. The symptoms of VKC have a seasonal pattern, although some patients develop a chronic form [<span>5</span>]. Topical antiallergic drugs may be effective for mild cases, while more severe cases require topical corticosteroids or immunosuppressant eye drops [<span>3, 6, 7</span>].</p><p>VKC may have a genetic substrate [<span>8, 9</span>], but recognizes in its pathophysiology an immunological involvement, with both IgE- and non-IgE-mediated mechanisms [<span>2, 10-12</span>].</p><p>Until now, the ocular cellular landscape has been characterized using different methods of tear collection (i.e., impression cytology, conjunctival brushing or biopsy, microcapillary or surgical sponge methods, aspiration techniques, or Schirmer test paper) [<span>13-16</span>].</p><p>We investigated the Schirmer test's potential uses to assess the conjunctival surface's immunological content. Among all the others, this test is the least bothersome and painful method of tear collection, especially in the pediatric population where it is routinely performed during the first-level ophthalmological evaluation in patients with VKC [<span>17</span>].</p><p>We studied 58 samples derived from VKC patients analyzed at diagnosis and/or during treatment, whose clinical and demographic characteristics are summarized in Table S1.</p><p>Cells collected from paper filters used in the Schirmer test (see Appendix S1) were enriched with leukocytes exhibiting low granularity (Figure 1A). We observed a significant increase in the absolute number, normalized by the size of the tears calculated with the Schirmer test itself, and percentages of leukocytes (CD45<sup>+</sup>cells) in inflamed ocular surfaces in untreated (group 1) compared with treated (group 2) VKC patients (Figure 1B). Among the treated patients (group 2), it was possible to identify, based on clinical characteristics (i.e., disappearance or attenuation of clinical symptoms) and by meta-analysis studies [<span>18</span>], a group of patients who did not respond (group 2-NR) and a group of patients who responded (group 2-R) to therapy. In particular, 2-NR patients displayed higher amounts and percentages of leukocytes than 2-R patients (Figure 1B). Highly activated leukocytes (% of CD45<sup>+</sup>HLA-DR<sup>+</sup>) were observed in group 1 compared to group 2 patients (Figure 1B). 2-NR patients showed a higher HLA-DR expression than 2-R patients, confirming the correlation between the activation status and the response to therapy (Figure 1B).</p><p>We specifically characterized the immune cell composition by analyzing specific markers to identify T-, B-, NK- cells, and monocytes (Figure 1C,D). Our data showed increased T-cell infiltration in untreated compared to treated VKC patients. Similarly, 2-NR patients displayed a higher frequency of T cells than 2-R patients (Figure 1E). No significant differences were observed regarding B cells, monocytes, and NK cells in all groups analyzed (Figure 1E).</p><p>In our cohort of pediatric VKC patients, we have defined different ranges to classify the pathological status and the response to therapy. Untreated patients presented more than 3000 CD45<sup>+</sup> cells infiltrated, treated 2-NR patients had more than 2000 CD45<sup>+</sup> cells, while 2-R patients did not exceed 300 CD45<sup>+</sup> cells (Figure 2A). Moreover, evaluating T cells can be a further marker to distinguish untreated and 2-NR versus 2-R patients (Figure 2B). Of note, the number of leukocytes directly correlates with the clinical classification (T, L, M) suggesting the importance of this tool for clinical purposes (Figure 2C).</p><p>The clinical applicability of the established ranges was further verified by analyzing leukocyte infiltration. Figure 2D shows two representative patients, examined at T1 after the end of the treatment with the first cycle of cyclosporine (CsA) and at T2, continuing or changing therapy. These two patients showed different responses to the CsA treatment at T1 (T1<sub>c</sub>); indeed, patient 1, who had at T1 high levels of leukocytes (Figure 2D, T1<sub>c</sub>), corresponding to the red area of Figure 2A (containing the two groups of patients 1 and 2-NR), displayed severe symptoms (Figure 2E, panels a-b). At T2, the symptoms were resolved (Figure 2E, panels c-d) with Tacrolimus-based eye drops treatment, with a consequent reduction of leukocyte infiltration (Figure 2D, T2<sub>t</sub>). Meanwhile, patient 2 at T1 had a leukocyte count (Figure 2D, T1<sub>c</sub> and 2E panels e-f) that fell within the green range in Figure 2A (corresponding to group 2-R), continued treatment with CsA, and at T2 achieved clinical resolution (Figure 2E, panels g-h), with a reduction in leukocyte numbers (Figure 2D, T2<sub>c</sub>). Similar results were observed when we evaluated the frequency of T cells (Figure S1).</p><p>Among patients treated with CsA, the ratio (> 1) of leukocytes (T2 vs. T1) highlighted that patients with the mixed form of the disease at T1 did not respond to the continuous CsA treatment (Figure 2F). These data could be helpful in suggesting a switching therapy from CsA to tacrolimus eye drops based on the evaluation of leukocyte number.</p><p>In conclusion, all these data suggest that the Schirmer test and clinical observation may be supportive in easily identifying an immune landscape useful for clinical purposes to classify VKC patients. Topical CsA and tacrolimus in allergic eye diseases are efficient in treating children and young patients affected by VKC [<span>7</span>]. However, previous literature indicates that the effectiveness of these topical treatments varies across different symptoms and signs, emphasizing the need for improved studies, consensus on core outcomes, and the potential for individualized therapy [<span>18</span>]. In this context, our study aims to characterize immune cells to enhance monitoring and establish a therapeutic regimen, or even discontinue therapy based on the number of leukocytes present.</p><p><b>Maria Teresa Bilotta:</b> methodology, formal analysis, investigation, data curation, writing – original draft, writing – review and editing. <b>Massimiliano Raponi:</b> writing-review and editing, formal analysis. <b>Mariacristina Esposito:</b> investigation, data curation. <b>Giuseppe Bianco:</b> methodology. <b>Luca Buzzonetti</b>, <b>Alessandro Giovanni Fiocchi</b>, and <b>Lorenzo Moretta:</b> writing – original draft, writing – review and editing, supervision. <b>Paola Vacca</b>, <b>Nicola Tumino</b>, and <b>Maria Cristina Artesani:</b> conceptualization, formal analysis, methodology, data curation, writing – original draft, writing – review and editing, supervision, funding acquisition, project administration, investigation.</p><p>The authors have nothing to report.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":122,\"journal\":{\"name\":\"Allergy\",\"volume\":\"80 7\",\"pages\":\"2050-2054\"},\"PeriodicalIF\":12.0000,\"publicationDate\":\"2025-03-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/all.16525\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/all.16525\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/all.16525","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
Immunophenotyping in Vernal Keratoconjunctivitis: Schirmer Test for Therapy Response Prediction
Vernal keratoconjunctivitis (VKC) is a disease of the anterior segment of the eye primarily affecting children. Diagnosis is confirmed by the evidence of signs such as an upper tarsal papillary reaction or limbal conjunctival nodules (Trantas dots) and is classified as tarsal (T) or limbal (L), respectively, or mixed (M) when both signs are present [1-4]. The symptoms of VKC have a seasonal pattern, although some patients develop a chronic form [5]. Topical antiallergic drugs may be effective for mild cases, while more severe cases require topical corticosteroids or immunosuppressant eye drops [3, 6, 7].
VKC may have a genetic substrate [8, 9], but recognizes in its pathophysiology an immunological involvement, with both IgE- and non-IgE-mediated mechanisms [2, 10-12].
Until now, the ocular cellular landscape has been characterized using different methods of tear collection (i.e., impression cytology, conjunctival brushing or biopsy, microcapillary or surgical sponge methods, aspiration techniques, or Schirmer test paper) [13-16].
We investigated the Schirmer test's potential uses to assess the conjunctival surface's immunological content. Among all the others, this test is the least bothersome and painful method of tear collection, especially in the pediatric population where it is routinely performed during the first-level ophthalmological evaluation in patients with VKC [17].
We studied 58 samples derived from VKC patients analyzed at diagnosis and/or during treatment, whose clinical and demographic characteristics are summarized in Table S1.
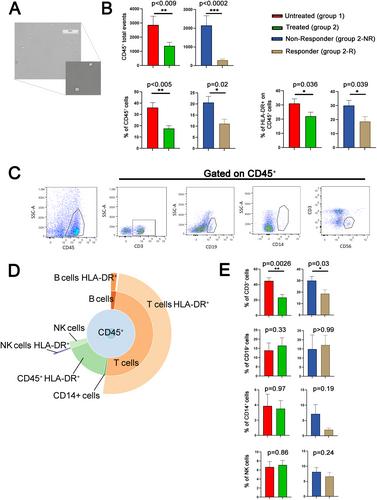
Cells collected from paper filters used in the Schirmer test (see Appendix S1) were enriched with leukocytes exhibiting low granularity (Figure 1A). We observed a significant increase in the absolute number, normalized by the size of the tears calculated with the Schirmer test itself, and percentages of leukocytes (CD45+cells) in inflamed ocular surfaces in untreated (group 1) compared with treated (group 2) VKC patients (Figure 1B). Among the treated patients (group 2), it was possible to identify, based on clinical characteristics (i.e., disappearance or attenuation of clinical symptoms) and by meta-analysis studies [18], a group of patients who did not respond (group 2-NR) and a group of patients who responded (group 2-R) to therapy. In particular, 2-NR patients displayed higher amounts and percentages of leukocytes than 2-R patients (Figure 1B). Highly activated leukocytes (% of CD45+HLA-DR+) were observed in group 1 compared to group 2 patients (Figure 1B). 2-NR patients showed a higher HLA-DR expression than 2-R patients, confirming the correlation between the activation status and the response to therapy (Figure 1B).
We specifically characterized the immune cell composition by analyzing specific markers to identify T-, B-, NK- cells, and monocytes (Figure 1C,D). Our data showed increased T-cell infiltration in untreated compared to treated VKC patients. Similarly, 2-NR patients displayed a higher frequency of T cells than 2-R patients (Figure 1E). No significant differences were observed regarding B cells, monocytes, and NK cells in all groups analyzed (Figure 1E).
In our cohort of pediatric VKC patients, we have defined different ranges to classify the pathological status and the response to therapy. Untreated patients presented more than 3000 CD45+ cells infiltrated, treated 2-NR patients had more than 2000 CD45+ cells, while 2-R patients did not exceed 300 CD45+ cells (Figure 2A). Moreover, evaluating T cells can be a further marker to distinguish untreated and 2-NR versus 2-R patients (Figure 2B). Of note, the number of leukocytes directly correlates with the clinical classification (T, L, M) suggesting the importance of this tool for clinical purposes (Figure 2C).
The clinical applicability of the established ranges was further verified by analyzing leukocyte infiltration. Figure 2D shows two representative patients, examined at T1 after the end of the treatment with the first cycle of cyclosporine (CsA) and at T2, continuing or changing therapy. These two patients showed different responses to the CsA treatment at T1 (T1c); indeed, patient 1, who had at T1 high levels of leukocytes (Figure 2D, T1c), corresponding to the red area of Figure 2A (containing the two groups of patients 1 and 2-NR), displayed severe symptoms (Figure 2E, panels a-b). At T2, the symptoms were resolved (Figure 2E, panels c-d) with Tacrolimus-based eye drops treatment, with a consequent reduction of leukocyte infiltration (Figure 2D, T2t). Meanwhile, patient 2 at T1 had a leukocyte count (Figure 2D, T1c and 2E panels e-f) that fell within the green range in Figure 2A (corresponding to group 2-R), continued treatment with CsA, and at T2 achieved clinical resolution (Figure 2E, panels g-h), with a reduction in leukocyte numbers (Figure 2D, T2c). Similar results were observed when we evaluated the frequency of T cells (Figure S1).
Among patients treated with CsA, the ratio (> 1) of leukocytes (T2 vs. T1) highlighted that patients with the mixed form of the disease at T1 did not respond to the continuous CsA treatment (Figure 2F). These data could be helpful in suggesting a switching therapy from CsA to tacrolimus eye drops based on the evaluation of leukocyte number.
In conclusion, all these data suggest that the Schirmer test and clinical observation may be supportive in easily identifying an immune landscape useful for clinical purposes to classify VKC patients. Topical CsA and tacrolimus in allergic eye diseases are efficient in treating children and young patients affected by VKC [7]. However, previous literature indicates that the effectiveness of these topical treatments varies across different symptoms and signs, emphasizing the need for improved studies, consensus on core outcomes, and the potential for individualized therapy [18]. In this context, our study aims to characterize immune cells to enhance monitoring and establish a therapeutic regimen, or even discontinue therapy based on the number of leukocytes present.
Maria Teresa Bilotta: methodology, formal analysis, investigation, data curation, writing – original draft, writing – review and editing. Massimiliano Raponi: writing-review and editing, formal analysis. Mariacristina Esposito: investigation, data curation. Giuseppe Bianco: methodology. Luca Buzzonetti, Alessandro Giovanni Fiocchi, and Lorenzo Moretta: writing – original draft, writing – review and editing, supervision. Paola Vacca, Nicola Tumino, and Maria Cristina Artesani: conceptualization, formal analysis, methodology, data curation, writing – original draft, writing – review and editing, supervision, funding acquisition, project administration, investigation.
期刊介绍:
Allergy is an international and multidisciplinary journal that aims to advance, impact, and communicate all aspects of the discipline of Allergy/Immunology. It publishes original articles, reviews, position papers, guidelines, editorials, news and commentaries, letters to the editors, and correspondences. The journal accepts articles based on their scientific merit and quality.
Allergy seeks to maintain contact between basic and clinical Allergy/Immunology and encourages contributions from contributors and readers from all countries. In addition to its publication, Allergy also provides abstracting and indexing information. Some of the databases that include Allergy abstracts are Abstracts on Hygiene & Communicable Disease, Academic Search Alumni Edition, AgBiotech News & Information, AGRICOLA Database, Biological Abstracts, PubMed Dietary Supplement Subset, and Global Health, among others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


