Farah Yasmin, Syeda Farwa Zaidi, Abdul Moeed, Maryam Shahzad, Muhammad Sohaib Asghar, Mahnoor Sadiq, Javed Iqbal, Salim Surani, M. Chadi Alraies
{"title":"急性冠脉综合征患者非元凶动脉立即与分期血运重建的临床结果:系统回顾和荟萃分析","authors":"Farah Yasmin, Syeda Farwa Zaidi, Abdul Moeed, Maryam Shahzad, Muhammad Sohaib Asghar, Mahnoor Sadiq, Javed Iqbal, Salim Surani, M. Chadi Alraies","doi":"10.1002/clc.70105","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Recent guidelines for acute coronary syndrome (ACS) with multivessel coronary artery disease (MVD) recommend revascularization of non-culprit lesions following primary percutaneous coronary intervention (PCI). However, the optimal timing for this procedure—whether immediate or staged—remains uncertain.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A comprehensive search using PubMed (MEDLINE), Cochrane Central, and Google Scholar was conducted to identify studies comparing clinical outcomes between immediate and staged revascularization approaches in patients with MVD undergoing PCI. A random effects model was used to calculate risk ratios (RRs) for dichotomous outcomes with 95% confidence intervals (CIs). The primary outcome was 1-year all-cause mortality.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 10 randomized controlled trials (RCTs), comprising 3886 patients (1964 in the immediate revascularization group and 1940 in the staged revascularization group), with a median follow-up of 12 months, were included in the analysis. No significant difference in the risk of 1-year mortality was noted between the two approaches. The risk of target vessel revascularization (TVR) at 1-year follow-up was significantly lower in the immediate revascularization group compared to the staged revascularization group (RR: 0.64; 95% CI: 0.47–0.86; I²: 0%; <i>p</i> = 0.03). Additionally, the immediate revascularization group had a significantly lower risk of myocardial infarction (MI) at 1-year follow-up than the staged approach (RR: 0.57; 95% CI: 0.37–0.88; I²: 10%; <i>p</i> = 0.01).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>This meta-analysis suggests that immediate revascularization is associated with a significantly lower risk of TVR and MI at 1-year compared to staged revascularization.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"48 3","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70105","citationCount":"0","resultStr":"{\"title\":\"Clinical Outcomes of Immediate Versus Staged Revascularization of Nonculprit Arteries in Patients With Acute Coronary Syndrome: A Systematic Review and Meta-Analysis\",\"authors\":\"Farah Yasmin, Syeda Farwa Zaidi, Abdul Moeed, Maryam Shahzad, Muhammad Sohaib Asghar, Mahnoor Sadiq, Javed Iqbal, Salim Surani, M. Chadi Alraies\",\"doi\":\"10.1002/clc.70105\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Recent guidelines for acute coronary syndrome (ACS) with multivessel coronary artery disease (MVD) recommend revascularization of non-culprit lesions following primary percutaneous coronary intervention (PCI). However, the optimal timing for this procedure—whether immediate or staged—remains uncertain.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A comprehensive search using PubMed (MEDLINE), Cochrane Central, and Google Scholar was conducted to identify studies comparing clinical outcomes between immediate and staged revascularization approaches in patients with MVD undergoing PCI. A random effects model was used to calculate risk ratios (RRs) for dichotomous outcomes with 95% confidence intervals (CIs). The primary outcome was 1-year all-cause mortality.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 10 randomized controlled trials (RCTs), comprising 3886 patients (1964 in the immediate revascularization group and 1940 in the staged revascularization group), with a median follow-up of 12 months, were included in the analysis. No significant difference in the risk of 1-year mortality was noted between the two approaches. The risk of target vessel revascularization (TVR) at 1-year follow-up was significantly lower in the immediate revascularization group compared to the staged revascularization group (RR: 0.64; 95% CI: 0.47–0.86; I²: 0%; <i>p</i> = 0.03). Additionally, the immediate revascularization group had a significantly lower risk of myocardial infarction (MI) at 1-year follow-up than the staged approach (RR: 0.57; 95% CI: 0.37–0.88; I²: 10%; <i>p</i> = 0.01).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>This meta-analysis suggests that immediate revascularization is associated with a significantly lower risk of TVR and MI at 1-year compared to staged revascularization.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"48 3\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-03-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70105\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.70105\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.70105","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Clinical Outcomes of Immediate Versus Staged Revascularization of Nonculprit Arteries in Patients With Acute Coronary Syndrome: A Systematic Review and Meta-Analysis
Background
Recent guidelines for acute coronary syndrome (ACS) with multivessel coronary artery disease (MVD) recommend revascularization of non-culprit lesions following primary percutaneous coronary intervention (PCI). However, the optimal timing for this procedure—whether immediate or staged—remains uncertain.
Methods
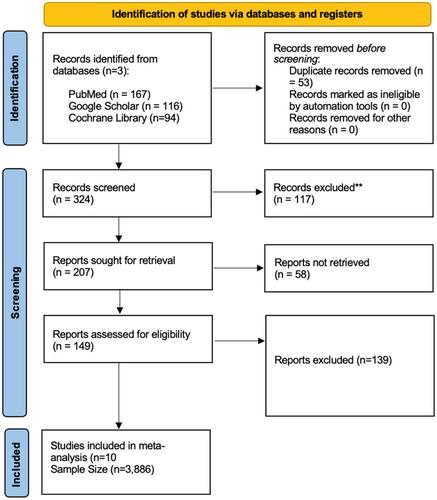
A comprehensive search using PubMed (MEDLINE), Cochrane Central, and Google Scholar was conducted to identify studies comparing clinical outcomes between immediate and staged revascularization approaches in patients with MVD undergoing PCI. A random effects model was used to calculate risk ratios (RRs) for dichotomous outcomes with 95% confidence intervals (CIs). The primary outcome was 1-year all-cause mortality.
Results
A total of 10 randomized controlled trials (RCTs), comprising 3886 patients (1964 in the immediate revascularization group and 1940 in the staged revascularization group), with a median follow-up of 12 months, were included in the analysis. No significant difference in the risk of 1-year mortality was noted between the two approaches. The risk of target vessel revascularization (TVR) at 1-year follow-up was significantly lower in the immediate revascularization group compared to the staged revascularization group (RR: 0.64; 95% CI: 0.47–0.86; I²: 0%; p = 0.03). Additionally, the immediate revascularization group had a significantly lower risk of myocardial infarction (MI) at 1-year follow-up than the staged approach (RR: 0.57; 95% CI: 0.37–0.88; I²: 10%; p = 0.01).
Conclusion
This meta-analysis suggests that immediate revascularization is associated with a significantly lower risk of TVR and MI at 1-year compared to staged revascularization.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


