Kewu Huang, Meishan Liu, Wenjun Wang, Honglei Shi, Chenxi Shi, Ying Wang, Eric D. Bateman, Yanming Li, Xiaokai Feng, Huahao Shen, Chen Wang
{"title":"中国哮喘患者哮喘预后不良的哮喘控制和危险因素:多中心单组研究(CARE4ALL)的基线分析","authors":"Kewu Huang, Meishan Liu, Wenjun Wang, Honglei Shi, Chenxi Shi, Ying Wang, Eric D. Bateman, Yanming Li, Xiaokai Feng, Huahao Shen, Chen Wang","doi":"10.1111/all.16522","DOIUrl":null,"url":null,"abstract":"<p>The prevalence of asthma among adults in China is 4.2%, affecting 45.7 million individuals, and is expected to increase due to environmental and lifestyle changes [<span>1</span>]. However, asthma control in China remains suboptimal: the well-controlled rates were reported at 28.7% in 2007–2008 and 28.5% in 2015–2016 [<span>2, 3</span>], and 61.6% of newly diagnosed asthma patients had severe persistent asthma [<span>4</span>], leading to a heavy disease burden manifested in frequent hospital admissions and emergency department visits due to exacerbations [<span>3</span>]. Although the underlying reasons may be manifold, low awareness of and adherence to Global Initiative for Asthma (GINA) recommendations among physicians and poor treatment adherence among patients both play a role [<span>5, 6</span>].</p><p>To improve asthma outcomes through aligning domestic clinical practice with international standards, we conducted a multi-centre single-arm study—CARE4ALL (NCT05440097), which undertook the first nationwide multifaceted quality improvement programme for asthma care. This baseline analysis assessed the overall asthma control level and investigated potential risk factors for not well-controlled asthma.</p><p>CARE4ALL recruited asthma outpatients aged ≥ 14 years from 8 secondary and 23 tertiary hospitals across most geographic areas in China. At the baseline visit, patients' demographics and asthma-related clinical characteristics were collected or assessed. Risk factors for not well-controlled asthma were identified through difference analyses between the ‘well and partly controlled’ group (Asthma Control Questionnaire [ACQ-5] < 1.5) and the ‘not well-controlled’ group (ACQ-5 ≥ 1.5) and multiple logistic regression (exploratory analysis without alpha adjustment).</p><p>During 2022–2023, 1500 patients were enrolled. At baseline, of the 1487 patients with recorded ACQ-5 scores, 728 (49.0%) had not well-controlled asthma (ACQ-5 ≥ 1.5), while 376 (25.3%) and 383 (25.8%) had well-controlled (ACQ-5 ≤ 0.75) and partly controlled (0.75 < ACQ-5 < 1.5) asthma, respectively. Of the 1500 enrolled patients, 461 (30.7%) had experienced at least one exacerbation in the 12 months preceding the baseline. Regarding asthma medication, 744 (49.6%) patients were not prescribed any asthma medication; among the 756 patients with asthma medications, 618 (81.7%) were prescribed inhaled corticosteroid (ICS)-containing medications, while the others were prescribed non-ICS medications, including leukotriene receptor antagonists (the commonest), short-acting beta-agonists and theophylline. When the clinical characteristics of the two groups by ACQ-5 were compared, the well and partly controlled group had better quality-of-life (assessed by Asthma Quality of Life Questionnaire [Standardised] for 12 years and older), better lung function and fewer exacerbations (Figure 1). Comparisons of the demographics and medication patterns between the two groups revealed significant inter-group differences in age, education level, household monthly income per capita, occupational exposure, residence area, hospital level and asthma medication use (Tables S2, S3). Subsequent multiple logistic regression revealed that an education level of elementary school or below (odds ratio [OR] = 2.14), occupational exposure to dust, allergens or harmful gases (OR = 1.66), and non-standard asthma treatment, including no medication prescription (OR = 1.37) and prescription of non-ICS-containing medication (OR = 2.15), were associated with not well-controlled asthma (Table 1).</p><p>A limitation of this study is that primary healthcare facilities in the rural areas of China were not included, which are known to be confronted with more severe issues of delayed information acquisition and medical resource shortage. Further research is needed to evaluate the quality of asthma care and control rates in these settings to improve overall asthma management in rural areas. Another limitation is the absence of patient phenotyping for Type-2/non-Type-2 inflammation, as the tests for blood eosinophil and fractional exhaled nitric oxide were optional in this study. Nonetheless, as ICS-containing medications are GINA-recommended treatments for asthma of all severity, we believe inflammation phenotyping is not essential for achieving the primary objective of this study.</p><p>In conclusion, our findings reflect current suboptimal asthma control in China, with half of the patients experiencing not well-controlled asthma and being more prone to frequent exacerbations and diminished health-related quality of life. We observed that certain demographic characteristics such as old age, low household income and residence in rural areas were more prevalent among patients with not well-controlled asthma, suggesting a need for focused management of these populations. Risk factors associated with not well-controlled asthma included low education level, occupational exposure to dust, allergens or harmful gases, and non-standard asthma treatment (no medication prescription or prescription of non-ICS-containing medication). The association between age and asthma control observed in our analysis is consistent with the finding from a previous domestic study, where age ≥ 45 years was identified as a predictor of uncontrolled asthma [<span>6</span>]. The adverse impact of ICS underuse on asthma control was also demonstrated in another Chinese study [<span>5</span>]. Notably, we observed a deviation in the prescription pattern of asthma medications from GINA recommendations, as approximately half of the patients were not prescribed any asthma medications, and among those who were, some were still prescribed non-ICS-containing regimens. These findings highlight the importance of enhancing physicians' proficiency in GINA recommendations and patient management skills to improve domestic asthma management, which is the focus of the recently completed CARE4ALL quality improvement programme.</p><p>All authors participated in the development of the study design and in the drafting and critical revision of the manuscript. All authors read and approved the final manuscript.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":122,"journal":{"name":"Allergy","volume":"80 5","pages":"1487-1490"},"PeriodicalIF":12.0000,"publicationDate":"2025-03-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/all.16522","citationCount":"0","resultStr":"{\"title\":\"Asthma Control and Risk Factors for Poor Asthma Outcomes in Chinese Asthma Patients: Baseline Analysis of a Multi-Centre, Single-Arm Study (CARE4ALL)\",\"authors\":\"Kewu Huang, Meishan Liu, Wenjun Wang, Honglei Shi, Chenxi Shi, Ying Wang, Eric D. Bateman, Yanming Li, Xiaokai Feng, Huahao Shen, Chen Wang\",\"doi\":\"10.1111/all.16522\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The prevalence of asthma among adults in China is 4.2%, affecting 45.7 million individuals, and is expected to increase due to environmental and lifestyle changes [<span>1</span>]. However, asthma control in China remains suboptimal: the well-controlled rates were reported at 28.7% in 2007–2008 and 28.5% in 2015–2016 [<span>2, 3</span>], and 61.6% of newly diagnosed asthma patients had severe persistent asthma [<span>4</span>], leading to a heavy disease burden manifested in frequent hospital admissions and emergency department visits due to exacerbations [<span>3</span>]. Although the underlying reasons may be manifold, low awareness of and adherence to Global Initiative for Asthma (GINA) recommendations among physicians and poor treatment adherence among patients both play a role [<span>5, 6</span>].</p><p>To improve asthma outcomes through aligning domestic clinical practice with international standards, we conducted a multi-centre single-arm study—CARE4ALL (NCT05440097), which undertook the first nationwide multifaceted quality improvement programme for asthma care. This baseline analysis assessed the overall asthma control level and investigated potential risk factors for not well-controlled asthma.</p><p>CARE4ALL recruited asthma outpatients aged ≥ 14 years from 8 secondary and 23 tertiary hospitals across most geographic areas in China. At the baseline visit, patients' demographics and asthma-related clinical characteristics were collected or assessed. Risk factors for not well-controlled asthma were identified through difference analyses between the ‘well and partly controlled’ group (Asthma Control Questionnaire [ACQ-5] < 1.5) and the ‘not well-controlled’ group (ACQ-5 ≥ 1.5) and multiple logistic regression (exploratory analysis without alpha adjustment).</p><p>During 2022–2023, 1500 patients were enrolled. At baseline, of the 1487 patients with recorded ACQ-5 scores, 728 (49.0%) had not well-controlled asthma (ACQ-5 ≥ 1.5), while 376 (25.3%) and 383 (25.8%) had well-controlled (ACQ-5 ≤ 0.75) and partly controlled (0.75 < ACQ-5 < 1.5) asthma, respectively. Of the 1500 enrolled patients, 461 (30.7%) had experienced at least one exacerbation in the 12 months preceding the baseline. Regarding asthma medication, 744 (49.6%) patients were not prescribed any asthma medication; among the 756 patients with asthma medications, 618 (81.7%) were prescribed inhaled corticosteroid (ICS)-containing medications, while the others were prescribed non-ICS medications, including leukotriene receptor antagonists (the commonest), short-acting beta-agonists and theophylline. When the clinical characteristics of the two groups by ACQ-5 were compared, the well and partly controlled group had better quality-of-life (assessed by Asthma Quality of Life Questionnaire [Standardised] for 12 years and older), better lung function and fewer exacerbations (Figure 1). Comparisons of the demographics and medication patterns between the two groups revealed significant inter-group differences in age, education level, household monthly income per capita, occupational exposure, residence area, hospital level and asthma medication use (Tables S2, S3). Subsequent multiple logistic regression revealed that an education level of elementary school or below (odds ratio [OR] = 2.14), occupational exposure to dust, allergens or harmful gases (OR = 1.66), and non-standard asthma treatment, including no medication prescription (OR = 1.37) and prescription of non-ICS-containing medication (OR = 2.15), were associated with not well-controlled asthma (Table 1).</p><p>A limitation of this study is that primary healthcare facilities in the rural areas of China were not included, which are known to be confronted with more severe issues of delayed information acquisition and medical resource shortage. Further research is needed to evaluate the quality of asthma care and control rates in these settings to improve overall asthma management in rural areas. Another limitation is the absence of patient phenotyping for Type-2/non-Type-2 inflammation, as the tests for blood eosinophil and fractional exhaled nitric oxide were optional in this study. Nonetheless, as ICS-containing medications are GINA-recommended treatments for asthma of all severity, we believe inflammation phenotyping is not essential for achieving the primary objective of this study.</p><p>In conclusion, our findings reflect current suboptimal asthma control in China, with half of the patients experiencing not well-controlled asthma and being more prone to frequent exacerbations and diminished health-related quality of life. We observed that certain demographic characteristics such as old age, low household income and residence in rural areas were more prevalent among patients with not well-controlled asthma, suggesting a need for focused management of these populations. Risk factors associated with not well-controlled asthma included low education level, occupational exposure to dust, allergens or harmful gases, and non-standard asthma treatment (no medication prescription or prescription of non-ICS-containing medication). The association between age and asthma control observed in our analysis is consistent with the finding from a previous domestic study, where age ≥ 45 years was identified as a predictor of uncontrolled asthma [<span>6</span>]. The adverse impact of ICS underuse on asthma control was also demonstrated in another Chinese study [<span>5</span>]. Notably, we observed a deviation in the prescription pattern of asthma medications from GINA recommendations, as approximately half of the patients were not prescribed any asthma medications, and among those who were, some were still prescribed non-ICS-containing regimens. These findings highlight the importance of enhancing physicians' proficiency in GINA recommendations and patient management skills to improve domestic asthma management, which is the focus of the recently completed CARE4ALL quality improvement programme.</p><p>All authors participated in the development of the study design and in the drafting and critical revision of the manuscript. All authors read and approved the final manuscript.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":122,\"journal\":{\"name\":\"Allergy\",\"volume\":\"80 5\",\"pages\":\"1487-1490\"},\"PeriodicalIF\":12.0000,\"publicationDate\":\"2025-03-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/all.16522\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/all.16522\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/all.16522","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
Asthma Control and Risk Factors for Poor Asthma Outcomes in Chinese Asthma Patients: Baseline Analysis of a Multi-Centre, Single-Arm Study (CARE4ALL)
The prevalence of asthma among adults in China is 4.2%, affecting 45.7 million individuals, and is expected to increase due to environmental and lifestyle changes [1]. However, asthma control in China remains suboptimal: the well-controlled rates were reported at 28.7% in 2007–2008 and 28.5% in 2015–2016 [2, 3], and 61.6% of newly diagnosed asthma patients had severe persistent asthma [4], leading to a heavy disease burden manifested in frequent hospital admissions and emergency department visits due to exacerbations [3]. Although the underlying reasons may be manifold, low awareness of and adherence to Global Initiative for Asthma (GINA) recommendations among physicians and poor treatment adherence among patients both play a role [5, 6].
To improve asthma outcomes through aligning domestic clinical practice with international standards, we conducted a multi-centre single-arm study—CARE4ALL (NCT05440097), which undertook the first nationwide multifaceted quality improvement programme for asthma care. This baseline analysis assessed the overall asthma control level and investigated potential risk factors for not well-controlled asthma.
CARE4ALL recruited asthma outpatients aged ≥ 14 years from 8 secondary and 23 tertiary hospitals across most geographic areas in China. At the baseline visit, patients' demographics and asthma-related clinical characteristics were collected or assessed. Risk factors for not well-controlled asthma were identified through difference analyses between the ‘well and partly controlled’ group (Asthma Control Questionnaire [ACQ-5] < 1.5) and the ‘not well-controlled’ group (ACQ-5 ≥ 1.5) and multiple logistic regression (exploratory analysis without alpha adjustment).
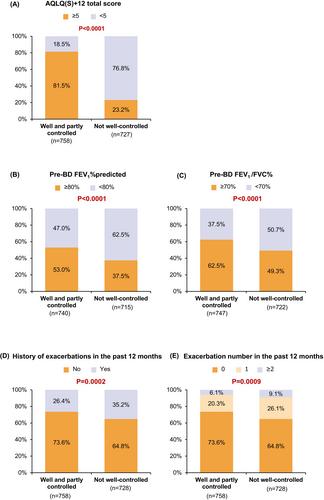
During 2022–2023, 1500 patients were enrolled. At baseline, of the 1487 patients with recorded ACQ-5 scores, 728 (49.0%) had not well-controlled asthma (ACQ-5 ≥ 1.5), while 376 (25.3%) and 383 (25.8%) had well-controlled (ACQ-5 ≤ 0.75) and partly controlled (0.75 < ACQ-5 < 1.5) asthma, respectively. Of the 1500 enrolled patients, 461 (30.7%) had experienced at least one exacerbation in the 12 months preceding the baseline. Regarding asthma medication, 744 (49.6%) patients were not prescribed any asthma medication; among the 756 patients with asthma medications, 618 (81.7%) were prescribed inhaled corticosteroid (ICS)-containing medications, while the others were prescribed non-ICS medications, including leukotriene receptor antagonists (the commonest), short-acting beta-agonists and theophylline. When the clinical characteristics of the two groups by ACQ-5 were compared, the well and partly controlled group had better quality-of-life (assessed by Asthma Quality of Life Questionnaire [Standardised] for 12 years and older), better lung function and fewer exacerbations (Figure 1). Comparisons of the demographics and medication patterns between the two groups revealed significant inter-group differences in age, education level, household monthly income per capita, occupational exposure, residence area, hospital level and asthma medication use (Tables S2, S3). Subsequent multiple logistic regression revealed that an education level of elementary school or below (odds ratio [OR] = 2.14), occupational exposure to dust, allergens or harmful gases (OR = 1.66), and non-standard asthma treatment, including no medication prescription (OR = 1.37) and prescription of non-ICS-containing medication (OR = 2.15), were associated with not well-controlled asthma (Table 1).
A limitation of this study is that primary healthcare facilities in the rural areas of China were not included, which are known to be confronted with more severe issues of delayed information acquisition and medical resource shortage. Further research is needed to evaluate the quality of asthma care and control rates in these settings to improve overall asthma management in rural areas. Another limitation is the absence of patient phenotyping for Type-2/non-Type-2 inflammation, as the tests for blood eosinophil and fractional exhaled nitric oxide were optional in this study. Nonetheless, as ICS-containing medications are GINA-recommended treatments for asthma of all severity, we believe inflammation phenotyping is not essential for achieving the primary objective of this study.
In conclusion, our findings reflect current suboptimal asthma control in China, with half of the patients experiencing not well-controlled asthma and being more prone to frequent exacerbations and diminished health-related quality of life. We observed that certain demographic characteristics such as old age, low household income and residence in rural areas were more prevalent among patients with not well-controlled asthma, suggesting a need for focused management of these populations. Risk factors associated with not well-controlled asthma included low education level, occupational exposure to dust, allergens or harmful gases, and non-standard asthma treatment (no medication prescription or prescription of non-ICS-containing medication). The association between age and asthma control observed in our analysis is consistent with the finding from a previous domestic study, where age ≥ 45 years was identified as a predictor of uncontrolled asthma [6]. The adverse impact of ICS underuse on asthma control was also demonstrated in another Chinese study [5]. Notably, we observed a deviation in the prescription pattern of asthma medications from GINA recommendations, as approximately half of the patients were not prescribed any asthma medications, and among those who were, some were still prescribed non-ICS-containing regimens. These findings highlight the importance of enhancing physicians' proficiency in GINA recommendations and patient management skills to improve domestic asthma management, which is the focus of the recently completed CARE4ALL quality improvement programme.
All authors participated in the development of the study design and in the drafting and critical revision of the manuscript. All authors read and approved the final manuscript.
期刊介绍:
Allergy is an international and multidisciplinary journal that aims to advance, impact, and communicate all aspects of the discipline of Allergy/Immunology. It publishes original articles, reviews, position papers, guidelines, editorials, news and commentaries, letters to the editors, and correspondences. The journal accepts articles based on their scientific merit and quality.
Allergy seeks to maintain contact between basic and clinical Allergy/Immunology and encourages contributions from contributors and readers from all countries. In addition to its publication, Allergy also provides abstracting and indexing information. Some of the databases that include Allergy abstracts are Abstracts on Hygiene & Communicable Disease, Academic Search Alumni Edition, AgBiotech News & Information, AGRICOLA Database, Biological Abstracts, PubMed Dietary Supplement Subset, and Global Health, among others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


