Jeroen P A Houwen, Arief Lalmohamed, Jochem Zwaan, Toine C G Egberts, Michiel Duyvendak, Aernoud T L Fiolet, Arend Mosterd
{"title":"秋水仙碱对使用维生素K拮抗剂的慢性冠心病患者凝血的影响。","authors":"Jeroen P A Houwen, Arief Lalmohamed, Jochem Zwaan, Toine C G Egberts, Michiel Duyvendak, Aernoud T L Fiolet, Arend Mosterd","doi":"10.1007/s00228-025-03815-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Low-dose (0.5 mg/day) colchicine improves cardiovascular outcomes in patients with stable coronary disease. Around 10-15% of these patients simultaneously use anticoagulant therapy, including vitamin-K antagonists (VKAs). In vitro studies and case reports have described a possible interaction between colchicine and VKAs leading to increased INR, but controlled studies are lacking.</p><p><strong>Objective: </strong>The aim of this study was to investigate if there is a drug-drug interaction between low-dose colchicine and VKAs in patients with chronic coronary disease.</p><p><strong>Methods: </strong>This study was a sub-analysis of the randomized low-dose colchicine for secondary prevention of cardiovascular disease 2 (LoDoCo2) trial. This placebo-controlled trial investigated efficacy of colchicine 0.5 mg once daily in patients with chronic coronary disease. For the current study, we included a selection of Dutch patients who concomitantly used a VKA. Following a 30 days open-label colchicine run-in phase, patients were randomized to colchicine or placebo. The primary outcome was the intra-patient difference in international normalized ratio (INR) during the first month after starting or stopping colchicine as compared to the preceding month. Secondary outcomes included changes in VKA daily dosage, assessed in the same pattern and before and after randomization, and time in therapeutic range (TTR), assessed before and after randomization to reflect long-term effects. INR measurements were part of routine clinical care.</p><p><strong>Results: </strong>In total, 73 patients were included (35 colchicine and 38 in the placebo group). No significant intra-patient change in INR was observed after starting colchicine during the open-label run-in phase (mean INR: 2.60 before vs. 2.67 during run-in, difference 0.07, 95% CI - 0.13 to 0.26; p = 0.50). Similarly, stopping colchicine treatment (i.e., randomization to placebo) did not significantly alter INR levels (mean INR: 2.70 during run-in vs. 2.81 after randomization, difference 0.11, 95% CI - 0.12 to 0.33; p = 0.34). The change in mean VKA daily dosage was - 0.01 mg (95% CI - 0.03 to 0.01; p = 0.35) when starting colchicine and - 0.01 mg (95% CI - 0.03 to 0.01; p = 0.41) when switching to placebo. TTR in patients allocated to active treatment was 65.8% in the year prior to the start of colchicine and 73.4% in the year after randomization to colchicine (change in TTR 7.56%, 95% CI - 0.14 to 15.26%; p = 0.05). Mean VKA dosage remained similar (change in VKA dosage of 0.01 mg; 95% CI - 0.11 to 0.13 mg; p = 0.84).</p><p><strong>Conclusion: </strong>No significant changes in INR, VKA dosage, or TTR in patients using VKAs after starting or stopping colchicine were observed. These results suggest that there is no need for additional INR monitoring beyond the standard of care when using low-dose colchicine, though further studies in larger populations would help to confirm this conclusion.</p>","PeriodicalId":11857,"journal":{"name":"European Journal of Clinical Pharmacology","volume":" ","pages":"719-725"},"PeriodicalIF":2.7000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12003603/pdf/","citationCount":"0","resultStr":"{\"title\":\"The effect of colchicine on coagulation in patients with chronic coronary disease who use vitamin K antagonists.\",\"authors\":\"Jeroen P A Houwen, Arief Lalmohamed, Jochem Zwaan, Toine C G Egberts, Michiel Duyvendak, Aernoud T L Fiolet, Arend Mosterd\",\"doi\":\"10.1007/s00228-025-03815-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Low-dose (0.5 mg/day) colchicine improves cardiovascular outcomes in patients with stable coronary disease. Around 10-15% of these patients simultaneously use anticoagulant therapy, including vitamin-K antagonists (VKAs). In vitro studies and case reports have described a possible interaction between colchicine and VKAs leading to increased INR, but controlled studies are lacking.</p><p><strong>Objective: </strong>The aim of this study was to investigate if there is a drug-drug interaction between low-dose colchicine and VKAs in patients with chronic coronary disease.</p><p><strong>Methods: </strong>This study was a sub-analysis of the randomized low-dose colchicine for secondary prevention of cardiovascular disease 2 (LoDoCo2) trial. This placebo-controlled trial investigated efficacy of colchicine 0.5 mg once daily in patients with chronic coronary disease. For the current study, we included a selection of Dutch patients who concomitantly used a VKA. Following a 30 days open-label colchicine run-in phase, patients were randomized to colchicine or placebo. The primary outcome was the intra-patient difference in international normalized ratio (INR) during the first month after starting or stopping colchicine as compared to the preceding month. Secondary outcomes included changes in VKA daily dosage, assessed in the same pattern and before and after randomization, and time in therapeutic range (TTR), assessed before and after randomization to reflect long-term effects. INR measurements were part of routine clinical care.</p><p><strong>Results: </strong>In total, 73 patients were included (35 colchicine and 38 in the placebo group). No significant intra-patient change in INR was observed after starting colchicine during the open-label run-in phase (mean INR: 2.60 before vs. 2.67 during run-in, difference 0.07, 95% CI - 0.13 to 0.26; p = 0.50). Similarly, stopping colchicine treatment (i.e., randomization to placebo) did not significantly alter INR levels (mean INR: 2.70 during run-in vs. 2.81 after randomization, difference 0.11, 95% CI - 0.12 to 0.33; p = 0.34). The change in mean VKA daily dosage was - 0.01 mg (95% CI - 0.03 to 0.01; p = 0.35) when starting colchicine and - 0.01 mg (95% CI - 0.03 to 0.01; p = 0.41) when switching to placebo. TTR in patients allocated to active treatment was 65.8% in the year prior to the start of colchicine and 73.4% in the year after randomization to colchicine (change in TTR 7.56%, 95% CI - 0.14 to 15.26%; p = 0.05). Mean VKA dosage remained similar (change in VKA dosage of 0.01 mg; 95% CI - 0.11 to 0.13 mg; p = 0.84).</p><p><strong>Conclusion: </strong>No significant changes in INR, VKA dosage, or TTR in patients using VKAs after starting or stopping colchicine were observed. These results suggest that there is no need for additional INR monitoring beyond the standard of care when using low-dose colchicine, though further studies in larger populations would help to confirm this conclusion.</p>\",\"PeriodicalId\":11857,\"journal\":{\"name\":\"European Journal of Clinical Pharmacology\",\"volume\":\" \",\"pages\":\"719-725\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12003603/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Clinical Pharmacology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00228-025-03815-9\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00228-025-03815-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
The effect of colchicine on coagulation in patients with chronic coronary disease who use vitamin K antagonists.
Background: Low-dose (0.5 mg/day) colchicine improves cardiovascular outcomes in patients with stable coronary disease. Around 10-15% of these patients simultaneously use anticoagulant therapy, including vitamin-K antagonists (VKAs). In vitro studies and case reports have described a possible interaction between colchicine and VKAs leading to increased INR, but controlled studies are lacking.
Objective: The aim of this study was to investigate if there is a drug-drug interaction between low-dose colchicine and VKAs in patients with chronic coronary disease.
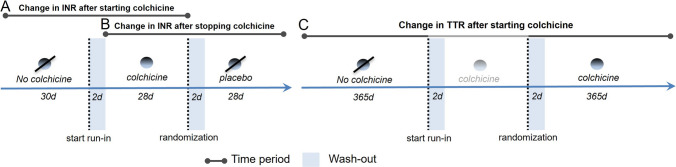
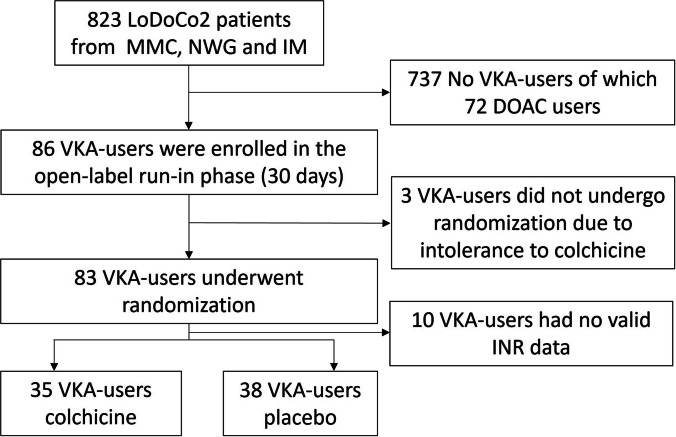
Methods: This study was a sub-analysis of the randomized low-dose colchicine for secondary prevention of cardiovascular disease 2 (LoDoCo2) trial. This placebo-controlled trial investigated efficacy of colchicine 0.5 mg once daily in patients with chronic coronary disease. For the current study, we included a selection of Dutch patients who concomitantly used a VKA. Following a 30 days open-label colchicine run-in phase, patients were randomized to colchicine or placebo. The primary outcome was the intra-patient difference in international normalized ratio (INR) during the first month after starting or stopping colchicine as compared to the preceding month. Secondary outcomes included changes in VKA daily dosage, assessed in the same pattern and before and after randomization, and time in therapeutic range (TTR), assessed before and after randomization to reflect long-term effects. INR measurements were part of routine clinical care.
Results: In total, 73 patients were included (35 colchicine and 38 in the placebo group). No significant intra-patient change in INR was observed after starting colchicine during the open-label run-in phase (mean INR: 2.60 before vs. 2.67 during run-in, difference 0.07, 95% CI - 0.13 to 0.26; p = 0.50). Similarly, stopping colchicine treatment (i.e., randomization to placebo) did not significantly alter INR levels (mean INR: 2.70 during run-in vs. 2.81 after randomization, difference 0.11, 95% CI - 0.12 to 0.33; p = 0.34). The change in mean VKA daily dosage was - 0.01 mg (95% CI - 0.03 to 0.01; p = 0.35) when starting colchicine and - 0.01 mg (95% CI - 0.03 to 0.01; p = 0.41) when switching to placebo. TTR in patients allocated to active treatment was 65.8% in the year prior to the start of colchicine and 73.4% in the year after randomization to colchicine (change in TTR 7.56%, 95% CI - 0.14 to 15.26%; p = 0.05). Mean VKA dosage remained similar (change in VKA dosage of 0.01 mg; 95% CI - 0.11 to 0.13 mg; p = 0.84).
Conclusion: No significant changes in INR, VKA dosage, or TTR in patients using VKAs after starting or stopping colchicine were observed. These results suggest that there is no need for additional INR monitoring beyond the standard of care when using low-dose colchicine, though further studies in larger populations would help to confirm this conclusion.
期刊介绍:
The European Journal of Clinical Pharmacology publishes original papers on all aspects of clinical pharmacology and drug therapy in humans. Manuscripts are welcomed on the following topics: therapeutic trials, pharmacokinetics/pharmacodynamics, pharmacogenetics, drug metabolism, adverse drug reactions, drug interactions, all aspects of drug development, development relating to teaching in clinical pharmacology, pharmacoepidemiology, and matters relating to the rational prescribing and safe use of drugs. Methodological contributions relevant to these topics are also welcomed.
Data from animal experiments are accepted only in the context of original data in man reported in the same paper. EJCP will only consider manuscripts describing the frequency of allelic variants in different populations if this information is linked to functional data or new interesting variants. Highly relevant differences in frequency with a major impact in drug therapy for the respective population may be submitted as a letter to the editor.
Straightforward phase I pharmacokinetic or pharmacodynamic studies as parts of new drug development will only be considered for publication if the paper involves
-a compound that is interesting and new in some basic or fundamental way, or
-methods that are original in some basic sense, or
-a highly unexpected outcome, or
-conclusions that are scientifically novel in some basic or fundamental sense.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


