Anselm Jorda, Lena Pracher, Sabine Eberl, Alina Nussbaumer-Pröll, Maysa Sarhan, Maria Weber, Markus Wahrmann, Valentin Al Jalali, Felix Bergmann, Marlene Prager, Amelie Leutzendorff, Maria Sanz-Codina, Lara Tegrovsky, Theresa Pecho, Bernd Jilma, Lena Müller, Andreas Spittler, Marianne Rocha-Hasler, Julia Eckl-Dorna, Anna Kusienicka, Matthias Farlik, Markus Zeitlinger
{"title":"细胞因子的稳定性,细胞和临床反应的静脉注射LPS挑战一年后重复:一个健康的志愿者试验。","authors":"Anselm Jorda, Lena Pracher, Sabine Eberl, Alina Nussbaumer-Pröll, Maysa Sarhan, Maria Weber, Markus Wahrmann, Valentin Al Jalali, Felix Bergmann, Marlene Prager, Amelie Leutzendorff, Maria Sanz-Codina, Lara Tegrovsky, Theresa Pecho, Bernd Jilma, Lena Müller, Andreas Spittler, Marianne Rocha-Hasler, Julia Eckl-Dorna, Anna Kusienicka, Matthias Farlik, Markus Zeitlinger","doi":"10.1007/s00430-025-00823-5","DOIUrl":null,"url":null,"abstract":"<p><p>Whether the magnitude of individual cytokine, cellular, and clinical responses to the intravenous lipopolysaccharide (LPS) challenge is constant in individuals over extended time periods is unknown. Nine healthy volunteers received an intravenous LPS injection of 2 ng/kg bodyweight twice at intervals of at least one year. Circulating cytokines and leukocyte subsets were quantified using a multiplex immunoassay and cytometry by time-of-flight, respectively. Self-reported symptoms and vital signs were also assessed. We observed moderate to strong intra-individual correlations in the responsiveness of most cytokines (IL-6 [AUC<sub>0 - 10</sub>]: R = 0.93, p < 0.001; CRP [mg/dL]: R = 0.88, p = 0.004; IL-8 [AUC<sub>0 - 10</sub>]: R = 0.71, p = 0.031; TNF-alpha [AUC<sub>0 - 10</sub>]: R = 0.67, p = 0.047; IL-10 [AUC<sub>0 - 10</sub>]: R = 0.42, p = 0.26) and cellular subsets (CD8 T lymphocytes: R = 0.9, p = 0.002; B lymphocytes [G/L]: R = 0.89, p = 0.003; CD4 T lymphocytes: R = 0.84, p = 0.001; neutrophils: R = 0.80, p = 0.017; monocytes: R = 0.16, p = 0.710) between the 1st and 2nd LPS challenges. Vital signs and symptoms were not reproducible. While the average cellular and clinical response was similar between the two LPS challenges, we found a significantly attenuated AUC<sub>0 - 10</sub> of IL-6 (percent difference, -41.9% [95% CI -73.0 - -10.7]) and TNF-alpha (percent difference, -35.7% [95% CI -70.0 - -1.6]) at the 2nd LPS challenge. Individual cytokine and cellular responses to intravenous LPS showed a significant degree of correlation when measured more than one year apart. These correlations did not translate to the reproducibility of clinical symptoms and vital signs, which showed greater variability and were not constant over time. The partly reduced cytokine release in the 2nd LPS challenge might be interpreted as an indicator of a long-lasting tolerance to endotoxin.</p>","PeriodicalId":18369,"journal":{"name":"Medical Microbiology and Immunology","volume":"214 1","pages":"14"},"PeriodicalIF":3.0000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11885351/pdf/","citationCount":"0","resultStr":"{\"title\":\"Stability of cytokine, cellular and clinical response to the intravenous LPS challenge repeated after one year: a healthy volunteer trial.\",\"authors\":\"Anselm Jorda, Lena Pracher, Sabine Eberl, Alina Nussbaumer-Pröll, Maysa Sarhan, Maria Weber, Markus Wahrmann, Valentin Al Jalali, Felix Bergmann, Marlene Prager, Amelie Leutzendorff, Maria Sanz-Codina, Lara Tegrovsky, Theresa Pecho, Bernd Jilma, Lena Müller, Andreas Spittler, Marianne Rocha-Hasler, Julia Eckl-Dorna, Anna Kusienicka, Matthias Farlik, Markus Zeitlinger\",\"doi\":\"10.1007/s00430-025-00823-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Whether the magnitude of individual cytokine, cellular, and clinical responses to the intravenous lipopolysaccharide (LPS) challenge is constant in individuals over extended time periods is unknown. Nine healthy volunteers received an intravenous LPS injection of 2 ng/kg bodyweight twice at intervals of at least one year. Circulating cytokines and leukocyte subsets were quantified using a multiplex immunoassay and cytometry by time-of-flight, respectively. Self-reported symptoms and vital signs were also assessed. We observed moderate to strong intra-individual correlations in the responsiveness of most cytokines (IL-6 [AUC<sub>0 - 10</sub>]: R = 0.93, p < 0.001; CRP [mg/dL]: R = 0.88, p = 0.004; IL-8 [AUC<sub>0 - 10</sub>]: R = 0.71, p = 0.031; TNF-alpha [AUC<sub>0 - 10</sub>]: R = 0.67, p = 0.047; IL-10 [AUC<sub>0 - 10</sub>]: R = 0.42, p = 0.26) and cellular subsets (CD8 T lymphocytes: R = 0.9, p = 0.002; B lymphocytes [G/L]: R = 0.89, p = 0.003; CD4 T lymphocytes: R = 0.84, p = 0.001; neutrophils: R = 0.80, p = 0.017; monocytes: R = 0.16, p = 0.710) between the 1st and 2nd LPS challenges. Vital signs and symptoms were not reproducible. While the average cellular and clinical response was similar between the two LPS challenges, we found a significantly attenuated AUC<sub>0 - 10</sub> of IL-6 (percent difference, -41.9% [95% CI -73.0 - -10.7]) and TNF-alpha (percent difference, -35.7% [95% CI -70.0 - -1.6]) at the 2nd LPS challenge. Individual cytokine and cellular responses to intravenous LPS showed a significant degree of correlation when measured more than one year apart. These correlations did not translate to the reproducibility of clinical symptoms and vital signs, which showed greater variability and were not constant over time. The partly reduced cytokine release in the 2nd LPS challenge might be interpreted as an indicator of a long-lasting tolerance to endotoxin.</p>\",\"PeriodicalId\":18369,\"journal\":{\"name\":\"Medical Microbiology and Immunology\",\"volume\":\"214 1\",\"pages\":\"14\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-03-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11885351/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Microbiology and Immunology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00430-025-00823-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Microbiology and Immunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00430-025-00823-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
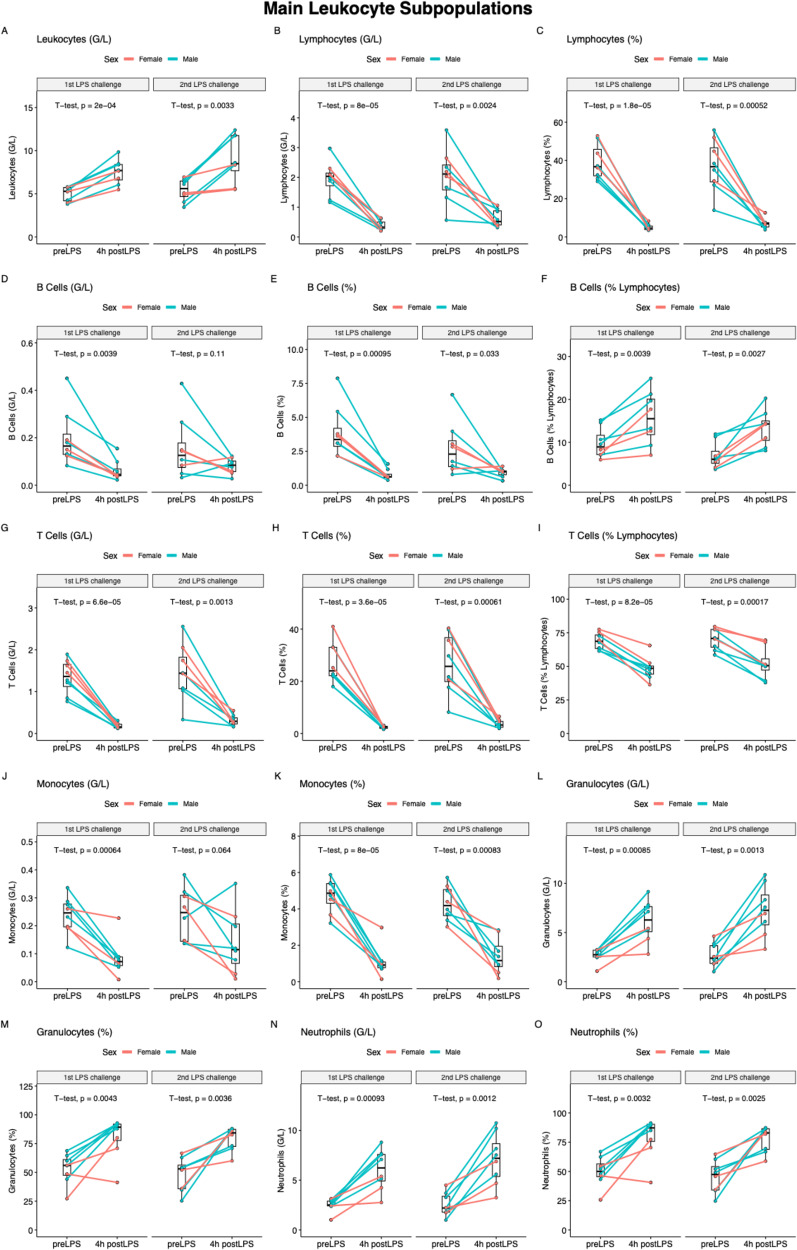
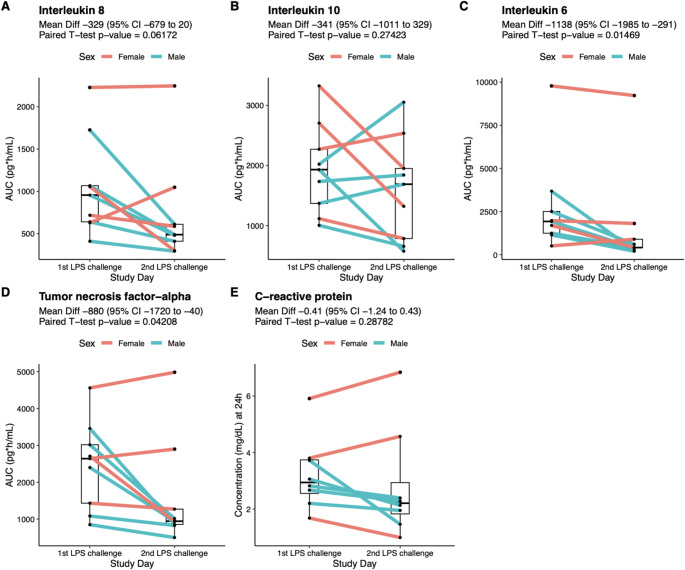
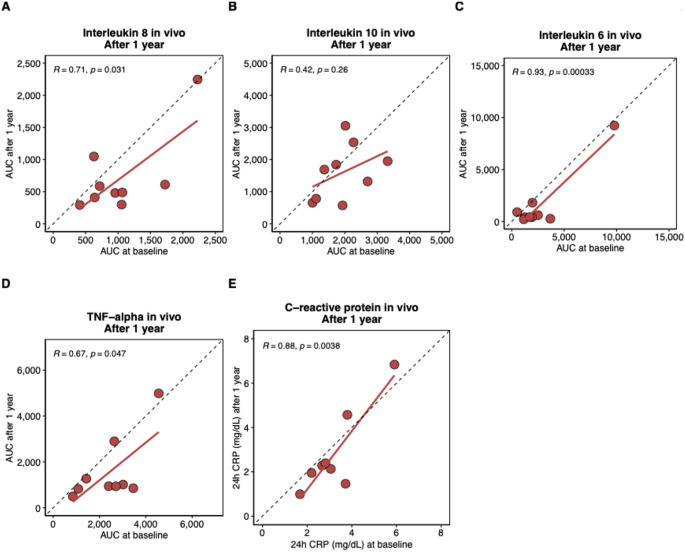
个体细胞因子、细胞和临床对静脉注射脂多糖(LPS)的反应在长时间内是否恒定是未知的。9名健康志愿者接受静脉注射2 ng/kg体重的LPS,间隔至少一年两次。循环细胞因子和白细胞亚群分别使用多重免疫分析法和飞行时间细胞术进行量化。自我报告的症状和生命体征也被评估。我们观察到大多数细胞因子的反应性在个体内具有中等到强烈的相关性(IL-6 [AUC0 - 10]: R = 0.93, p 0 - 10]: R = 0.71, p = 0.031;tnf - α [AUC0 - 10]: R = 0.67, p = 0.047;IL-10 [AUC0 -10]: R = 0.42, p = 0.26)和细胞亚群(CD8 T淋巴细胞:R = 0.9, p = 0.002;B淋巴细胞[G/L]: R = 0.89, p = 0.003;CD4 T淋巴细胞:R = 0.84, p = 0.001;中性粒细胞:R = 0.80, p = 0.017;单核细胞:R = 0.16, p = 0.710)。生命体征和症状不可重现。虽然两次LPS攻击的平均细胞和临床反应相似,但我们发现在第二次LPS攻击时,IL-6的AUC0 -10(差异百分比,-41.9% [95% CI -73.0 - -10.7])和tnf - α(差异百分比,-35.7% [95% CI -70.0 - -1.6])显著降低。个体细胞因子和细胞对静脉注射LPS的反应在相隔一年以上的时间内显示出显著的相关性。这些相关性并没有转化为临床症状和生命体征的可重复性,它们表现出更大的可变性,并且随着时间的推移不是恒定的。在第二次LPS刺激中部分减少的细胞因子释放可能被解释为对内毒素持久耐受的一个指标。
Stability of cytokine, cellular and clinical response to the intravenous LPS challenge repeated after one year: a healthy volunteer trial.
Whether the magnitude of individual cytokine, cellular, and clinical responses to the intravenous lipopolysaccharide (LPS) challenge is constant in individuals over extended time periods is unknown. Nine healthy volunteers received an intravenous LPS injection of 2 ng/kg bodyweight twice at intervals of at least one year. Circulating cytokines and leukocyte subsets were quantified using a multiplex immunoassay and cytometry by time-of-flight, respectively. Self-reported symptoms and vital signs were also assessed. We observed moderate to strong intra-individual correlations in the responsiveness of most cytokines (IL-6 [AUC0 - 10]: R = 0.93, p < 0.001; CRP [mg/dL]: R = 0.88, p = 0.004; IL-8 [AUC0 - 10]: R = 0.71, p = 0.031; TNF-alpha [AUC0 - 10]: R = 0.67, p = 0.047; IL-10 [AUC0 - 10]: R = 0.42, p = 0.26) and cellular subsets (CD8 T lymphocytes: R = 0.9, p = 0.002; B lymphocytes [G/L]: R = 0.89, p = 0.003; CD4 T lymphocytes: R = 0.84, p = 0.001; neutrophils: R = 0.80, p = 0.017; monocytes: R = 0.16, p = 0.710) between the 1st and 2nd LPS challenges. Vital signs and symptoms were not reproducible. While the average cellular and clinical response was similar between the two LPS challenges, we found a significantly attenuated AUC0 - 10 of IL-6 (percent difference, -41.9% [95% CI -73.0 - -10.7]) and TNF-alpha (percent difference, -35.7% [95% CI -70.0 - -1.6]) at the 2nd LPS challenge. Individual cytokine and cellular responses to intravenous LPS showed a significant degree of correlation when measured more than one year apart. These correlations did not translate to the reproducibility of clinical symptoms and vital signs, which showed greater variability and were not constant over time. The partly reduced cytokine release in the 2nd LPS challenge might be interpreted as an indicator of a long-lasting tolerance to endotoxin.
期刊介绍:
Medical Microbiology and Immunology (MMIM) publishes key findings on all aspects of the interrelationship between infectious agents and the immune system of their hosts. The journal´s main focus is original research work on intrinsic, innate or adaptive immune responses to viral, bacterial, fungal and parasitic (protozoan and helminthic) infections and on the virulence of the respective infectious pathogens.
MMIM covers basic, translational as well as clinical research in infectious diseases and infectious disease immunology. Basic research using cell cultures, organoid, and animal models are welcome, provided that the models have a clinical correlate and address a relevant medical question.
The journal also considers manuscripts on the epidemiology of infectious diseases, including the emergence and epidemic spreading of pathogens and the development of resistance to anti-infective therapies, and on novel vaccines and other innovative measurements of prevention.
The following categories of manuscripts will not be considered for publication in MMIM:
submissions of preliminary work, of merely descriptive data sets without investigation of mechanisms or of limited global interest,
manuscripts on existing or novel anti-infective compounds, which focus on pharmaceutical or pharmacological aspects of the drugs,
manuscripts on existing or modified vaccines, unless they report on experimental or clinical efficacy studies or provide new immunological information on their mode of action,
manuscripts on the diagnostics of infectious diseases, unless they offer a novel concept to solve a pending diagnostic problem,
case reports or case series, unless they are embedded in a study that focuses on the anti-infectious immune response and/or on the virulence of a pathogen.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


