{"title":"平均血小板体积、中性粒细胞与淋巴细胞比值、血小板与淋巴细胞比值对迟发性新生儿脓毒症的诊断价值。","authors":"Behzad Barekatain, Elahe Mardani, Alireza Sadeghnia, Zahra Heidari","doi":"10.4103/ijpvm.ijpvm_45_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neonatal sepsis (NS) is the most common cause of neonatal mortality, currently confirmed with blood culture as the diagnostic gold standard. However, being time-consuming, false-negative results, being affected by even a single dose of antibiotics, and expensiveness are negative aspects. Therefore, we aimed to investigate the diagnostic value of complete blood count (CBC) parameters: mean platelet volume (MPV), neutrophil-to-lymphocyte ratio (NLR), and platelet to lymphocyte ratio (PLR) which have been suggested in previous studies.</p><p><strong>Methods: </strong>A total of 100 term and preterm neonates (age ≥ 32 weeks) hospitalized in Alzahra and Shahid Beheshti hospitals in Isfahan, Iran, were studied. Fifty neonates with late neonatal sepsis were placed in the case group, and 50 neonates with other diagnoses were placed in the control group. Neonatal blood samples were sent to the laboratory, and MPV, NLR, and PLR were measured.</p><p><strong>Results: </strong>The mean (standard deviation) of MPV was 7.20 (4.39) in the case group and 9.55 (0.87) in the control group, and there was a significant difference between them (<i>P</i> value = 0.001). At the cutoff point of 8.25 in MPV, the area under the curve (AUC) was 0.594 with a sensitivity of 100% and specificity of 30%. The mean (standard deviation) of NLR was 1.79 (1.21) in the case group and 2.28 (1.25) in the control group, and there was no significant difference between them (<i>P</i> value = 0.692). The mean (standard deviation) of PLR was 62.58 (34.57) in the case group and 65.11 (28.55) in the control group, and there was no significant difference between them (<i>P</i> value = 0.836).</p><p><strong>Conclusions: </strong>MPV, unlike NLR and PLR, can be used as a sensitive and cost-effective primary screening index in late NS at the cutoff point of 8.25 due. However, low specificity suggests a poor diagnostic value.</p>","PeriodicalId":14342,"journal":{"name":"International Journal of Preventive Medicine","volume":"16 ","pages":"1"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11878645/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic Value of Mean Platelet Volume, Neutrophil-to-Lymphocyte Ratio, and Platelet to Lymphocyte Ratio for Late-Onset Neonatal Sepsis.\",\"authors\":\"Behzad Barekatain, Elahe Mardani, Alireza Sadeghnia, Zahra Heidari\",\"doi\":\"10.4103/ijpvm.ijpvm_45_23\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neonatal sepsis (NS) is the most common cause of neonatal mortality, currently confirmed with blood culture as the diagnostic gold standard. However, being time-consuming, false-negative results, being affected by even a single dose of antibiotics, and expensiveness are negative aspects. Therefore, we aimed to investigate the diagnostic value of complete blood count (CBC) parameters: mean platelet volume (MPV), neutrophil-to-lymphocyte ratio (NLR), and platelet to lymphocyte ratio (PLR) which have been suggested in previous studies.</p><p><strong>Methods: </strong>A total of 100 term and preterm neonates (age ≥ 32 weeks) hospitalized in Alzahra and Shahid Beheshti hospitals in Isfahan, Iran, were studied. Fifty neonates with late neonatal sepsis were placed in the case group, and 50 neonates with other diagnoses were placed in the control group. Neonatal blood samples were sent to the laboratory, and MPV, NLR, and PLR were measured.</p><p><strong>Results: </strong>The mean (standard deviation) of MPV was 7.20 (4.39) in the case group and 9.55 (0.87) in the control group, and there was a significant difference between them (<i>P</i> value = 0.001). At the cutoff point of 8.25 in MPV, the area under the curve (AUC) was 0.594 with a sensitivity of 100% and specificity of 30%. The mean (standard deviation) of NLR was 1.79 (1.21) in the case group and 2.28 (1.25) in the control group, and there was no significant difference between them (<i>P</i> value = 0.692). The mean (standard deviation) of PLR was 62.58 (34.57) in the case group and 65.11 (28.55) in the control group, and there was no significant difference between them (<i>P</i> value = 0.836).</p><p><strong>Conclusions: </strong>MPV, unlike NLR and PLR, can be used as a sensitive and cost-effective primary screening index in late NS at the cutoff point of 8.25 due. However, low specificity suggests a poor diagnostic value.</p>\",\"PeriodicalId\":14342,\"journal\":{\"name\":\"International Journal of Preventive Medicine\",\"volume\":\"16 \",\"pages\":\"1\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-01-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11878645/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Preventive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ijpvm.ijpvm_45_23\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Preventive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ijpvm.ijpvm_45_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Diagnostic Value of Mean Platelet Volume, Neutrophil-to-Lymphocyte Ratio, and Platelet to Lymphocyte Ratio for Late-Onset Neonatal Sepsis.
Background: Neonatal sepsis (NS) is the most common cause of neonatal mortality, currently confirmed with blood culture as the diagnostic gold standard. However, being time-consuming, false-negative results, being affected by even a single dose of antibiotics, and expensiveness are negative aspects. Therefore, we aimed to investigate the diagnostic value of complete blood count (CBC) parameters: mean platelet volume (MPV), neutrophil-to-lymphocyte ratio (NLR), and platelet to lymphocyte ratio (PLR) which have been suggested in previous studies.
Methods: A total of 100 term and preterm neonates (age ≥ 32 weeks) hospitalized in Alzahra and Shahid Beheshti hospitals in Isfahan, Iran, were studied. Fifty neonates with late neonatal sepsis were placed in the case group, and 50 neonates with other diagnoses were placed in the control group. Neonatal blood samples were sent to the laboratory, and MPV, NLR, and PLR were measured.
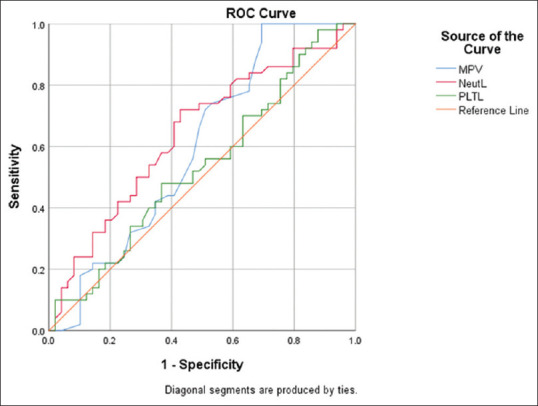
Results: The mean (standard deviation) of MPV was 7.20 (4.39) in the case group and 9.55 (0.87) in the control group, and there was a significant difference between them (P value = 0.001). At the cutoff point of 8.25 in MPV, the area under the curve (AUC) was 0.594 with a sensitivity of 100% and specificity of 30%. The mean (standard deviation) of NLR was 1.79 (1.21) in the case group and 2.28 (1.25) in the control group, and there was no significant difference between them (P value = 0.692). The mean (standard deviation) of PLR was 62.58 (34.57) in the case group and 65.11 (28.55) in the control group, and there was no significant difference between them (P value = 0.836).
Conclusions: MPV, unlike NLR and PLR, can be used as a sensitive and cost-effective primary screening index in late NS at the cutoff point of 8.25 due. However, low specificity suggests a poor diagnostic value.
期刊介绍:
International Journal of Preventive Medicine, a publication of Isfahan University of Medical Sciences, is a peer-reviewed online journal with Continuous print on demand compilation of issues published. The journal’s full text is available online at http://www.ijpvmjournal.net. The journal allows free access (Open Access) to its contents and permits authors to self-archive final accepted version of the articles on any OAI-compliant institutional / subject-based repository. The journal will cover technical and clinical studies related to health, ethical and social issues in field of Preventive Medicine. Articles with clinical interest and implications will be given preference.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


