Justin Dreyer, Lauren Kiryakoza, Jonathan Tijerina, Thomas Albini, Guillermo Amescua
{"title":"罕见双侧角膜巩膜穿孔继发于眼结核:1例报告及临床观察。","authors":"Justin Dreyer, Lauren Kiryakoza, Jonathan Tijerina, Thomas Albini, Guillermo Amescua","doi":"10.1186/s12348-025-00472-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This case represents a rare presentation of bilateral corneoscleral perforation secondary to presumed ocular mycobacterium tuberculosis infection with the goal of reporting a case of bilateral corneoscleral perforation in the setting of a positive interferon-γ release assay (IGRA) test.</p><p><strong>Findings: </strong>A 27-year-old patient presented with five months of redness, worsening eye pain, and five days of decreasing vision. Visual acuity (VA) was counting fingers bilaterally. Intraocular pressure (IOP) was 10 mmHg and 19 mmHg in the right and left eye, respectively. A slit lamp examination disclosed conjunctival injection, corneal haze, bilateral mutton-fat keratic precipitates, and a hypopyon in both eyes. The right eye had a 1.5 mm × 1.5 mm Seidel-positive corneal perforation with uveal prolapse. Similarly, the left eye had a 0.5 mm × 0.5 mm Seidel-negative inferior corneal perforation with uveal plugging. The chest X-ray showed a left-sided pleural effusion.</p><p><strong>Conclusion: </strong>Computed tomography (CT) of the face and sinuses showed bilateral circumferential globe thickening. IGRA was positive. All other rheumatologic and infectious workups were negative, including HIV, ACE, ANA, ANCA, CRP, anti-scleroderma antibody and HCV. The patient was treated with intravenous methylprednisolone and seven months of rifampin, isoniazid, pyrazinamide, and ethambutol. This workup shows the rare bilateral corneal involvement of ocular tuberculosis.</p>","PeriodicalId":16600,"journal":{"name":"Journal of Ophthalmic Inflammation and Infection","volume":"15 1","pages":"16"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11880446/pdf/","citationCount":"0","resultStr":"{\"title\":\"Rare bilateral corneoscleral perforation secondary to ocular tuberculosis: a case report and clinical insights.\",\"authors\":\"Justin Dreyer, Lauren Kiryakoza, Jonathan Tijerina, Thomas Albini, Guillermo Amescua\",\"doi\":\"10.1186/s12348-025-00472-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This case represents a rare presentation of bilateral corneoscleral perforation secondary to presumed ocular mycobacterium tuberculosis infection with the goal of reporting a case of bilateral corneoscleral perforation in the setting of a positive interferon-γ release assay (IGRA) test.</p><p><strong>Findings: </strong>A 27-year-old patient presented with five months of redness, worsening eye pain, and five days of decreasing vision. Visual acuity (VA) was counting fingers bilaterally. Intraocular pressure (IOP) was 10 mmHg and 19 mmHg in the right and left eye, respectively. A slit lamp examination disclosed conjunctival injection, corneal haze, bilateral mutton-fat keratic precipitates, and a hypopyon in both eyes. The right eye had a 1.5 mm × 1.5 mm Seidel-positive corneal perforation with uveal prolapse. Similarly, the left eye had a 0.5 mm × 0.5 mm Seidel-negative inferior corneal perforation with uveal plugging. The chest X-ray showed a left-sided pleural effusion.</p><p><strong>Conclusion: </strong>Computed tomography (CT) of the face and sinuses showed bilateral circumferential globe thickening. IGRA was positive. All other rheumatologic and infectious workups were negative, including HIV, ACE, ANA, ANCA, CRP, anti-scleroderma antibody and HCV. The patient was treated with intravenous methylprednisolone and seven months of rifampin, isoniazid, pyrazinamide, and ethambutol. This workup shows the rare bilateral corneal involvement of ocular tuberculosis.</p>\",\"PeriodicalId\":16600,\"journal\":{\"name\":\"Journal of Ophthalmic Inflammation and Infection\",\"volume\":\"15 1\",\"pages\":\"16\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-03-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11880446/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Ophthalmic Inflammation and Infection\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s12348-025-00472-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OPHTHALMOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Ophthalmic Inflammation and Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12348-025-00472-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:本病例是一例罕见的双侧角膜巩膜穿孔,继发于假定的眼部结核分枝杆菌感染,目的是报告一例干扰素-γ释放试验(IGRA)阳性的双侧角膜巩膜穿孔。结果:27岁的患者表现为5个月的红肿,眼部疼痛加重,5天视力下降。视敏度(VA)为双侧手指数。右眼和左眼眼压分别为10 mmHg和19 mmHg。裂隙灯检查发现结膜注射,角膜混浊,双侧羊脂角质沉淀,双眼低视。右眼有一个1.5 mm × 1.5 mm的seidel阳性角膜穿孔伴葡萄膜脱垂。同样,左眼有0.5 mm × 0.5 mm seidel阴性下角膜穿孔伴葡萄膜堵塞。胸部x光片显示左侧胸腔积液。结论:面部及鼻窦CT表现为双侧周向球增厚。IGRA阳性。所有其他风湿病和传染病检查均为阴性,包括HIV、ACE、ANA、ANCA、CRP、抗硬皮病抗体和HCV。患者静脉注射甲基强的松龙和7个月的利福平、异烟肼、吡嗪酰胺和乙胺丁醇。本检查显示罕见的双侧角膜累及眼结核。
Rare bilateral corneoscleral perforation secondary to ocular tuberculosis: a case report and clinical insights.
Background: This case represents a rare presentation of bilateral corneoscleral perforation secondary to presumed ocular mycobacterium tuberculosis infection with the goal of reporting a case of bilateral corneoscleral perforation in the setting of a positive interferon-γ release assay (IGRA) test.
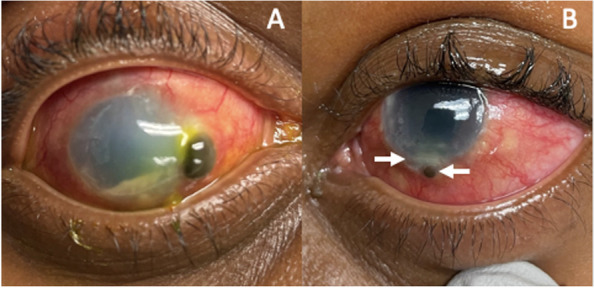
Findings: A 27-year-old patient presented with five months of redness, worsening eye pain, and five days of decreasing vision. Visual acuity (VA) was counting fingers bilaterally. Intraocular pressure (IOP) was 10 mmHg and 19 mmHg in the right and left eye, respectively. A slit lamp examination disclosed conjunctival injection, corneal haze, bilateral mutton-fat keratic precipitates, and a hypopyon in both eyes. The right eye had a 1.5 mm × 1.5 mm Seidel-positive corneal perforation with uveal prolapse. Similarly, the left eye had a 0.5 mm × 0.5 mm Seidel-negative inferior corneal perforation with uveal plugging. The chest X-ray showed a left-sided pleural effusion.
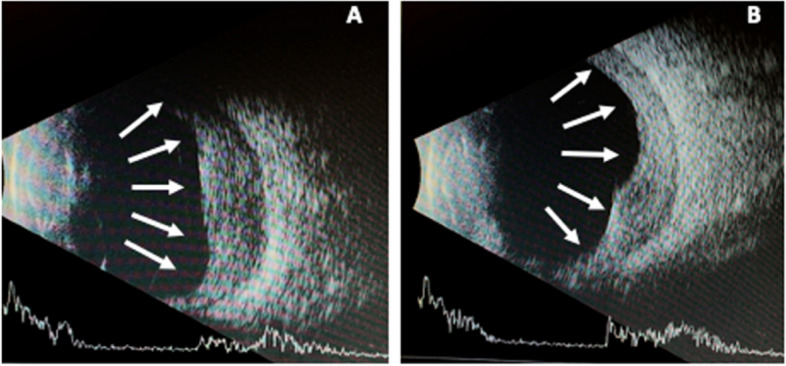
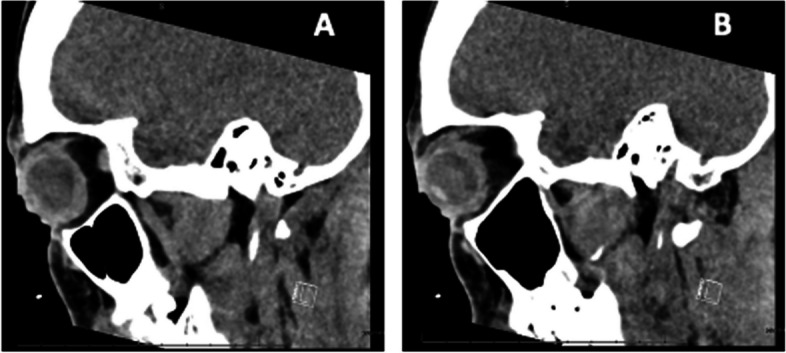
Conclusion: Computed tomography (CT) of the face and sinuses showed bilateral circumferential globe thickening. IGRA was positive. All other rheumatologic and infectious workups were negative, including HIV, ACE, ANA, ANCA, CRP, anti-scleroderma antibody and HCV. The patient was treated with intravenous methylprednisolone and seven months of rifampin, isoniazid, pyrazinamide, and ethambutol. This workup shows the rare bilateral corneal involvement of ocular tuberculosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


