{"title":"胸腔镜食管切除术中右上肺静脉位置对隆突下淋巴结清扫的影响:1例报告并文献复习。","authors":"Takeshi Horaguchi, Yuta Sato, Yuji Hatanaka, Yoshihiro Tanaka, Noriki Mitsui, Masahiro Fukada, Itaru Yasufuku, Ryuichi Asai, Jesse Yu Tajima, Nobuhisa Matsuhashi","doi":"10.70352/scrj.cr.24-0093","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The right top pulmonary vein (RTPV) is a rare anatomical variant that arises independently of the right superior lobe. It drains behind the right main bronchus or bronchus intermedius and into the left atrium or another pulmonary vein. This anomaly poses challenges during subcarinal lymph node dissection in thoracic surgery, such as esophagectomy, owing to the risk of vascular injury. The RTPV is mainly located behind the right main bronchus and right intermediate bronchus; however, reports of subcarinal dissection focusing on these sites are lacking. Herein, we present a case of esophageal cancer with an RTPV that was treated with thoracoscopic esophagectomy and propose a convenient classification for the anatomical findings and RTPV site.</p><p><strong>Case presentation: </strong>A 71-year-old man underwent a thoracoscopic esophagectomy for esophageal cancer (T1bN0M0) during a routine medical checkup. A preoperative computed tomography scan revealed an anomaly in which the RTPV drained into the left atrium behind the right main bronchus. Radical subcarinal lymphadenectomy was performed while preserving the RTPV, using 3 dimensions for preoperative simulation and intraoperative navigation. The operation lasted 6 h and 42 min, and the blood loss volume was 30 mL. The patient's postoperative course was uneventful, and he was discharged on postoperative day 21.</p><p><strong>Conclusions: </strong>In a retrospective review of esophageal cancer surgery cases at our hospital, RTPV was observed in 17/314 cases (5.4%). The most common inflow site was the inferior pulmonary vein (IPV) (9 cases), followed by the left atrium (5 cases), superior pulmonary vein (2 cases), and superior branch of the IPV (1 case). The inflow site was behind the right main bronchus and the right intermediate bronchus in 4 and 13 cases, respectively. Compared to past reviews, the inflow site varied somewhat; however, the vascular location remained the same. By classifying the areas behind the right main and right intermediate bronchi as Zones 1 and 2, respectively, cases in which the RTPV runs through Zone 1, as identified on preoperative computed tomography, should be manipulated with caution due to the risk of injury during lymph node dissection beneath the tracheal bifurcation.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11873321/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Right Top Pulmonary Vein Location on Subcarinal Lymph Node Dissection in Thoracoscopic Esophagectomy: A Case Report and Literature Review.\",\"authors\":\"Takeshi Horaguchi, Yuta Sato, Yuji Hatanaka, Yoshihiro Tanaka, Noriki Mitsui, Masahiro Fukada, Itaru Yasufuku, Ryuichi Asai, Jesse Yu Tajima, Nobuhisa Matsuhashi\",\"doi\":\"10.70352/scrj.cr.24-0093\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The right top pulmonary vein (RTPV) is a rare anatomical variant that arises independently of the right superior lobe. It drains behind the right main bronchus or bronchus intermedius and into the left atrium or another pulmonary vein. This anomaly poses challenges during subcarinal lymph node dissection in thoracic surgery, such as esophagectomy, owing to the risk of vascular injury. The RTPV is mainly located behind the right main bronchus and right intermediate bronchus; however, reports of subcarinal dissection focusing on these sites are lacking. Herein, we present a case of esophageal cancer with an RTPV that was treated with thoracoscopic esophagectomy and propose a convenient classification for the anatomical findings and RTPV site.</p><p><strong>Case presentation: </strong>A 71-year-old man underwent a thoracoscopic esophagectomy for esophageal cancer (T1bN0M0) during a routine medical checkup. A preoperative computed tomography scan revealed an anomaly in which the RTPV drained into the left atrium behind the right main bronchus. Radical subcarinal lymphadenectomy was performed while preserving the RTPV, using 3 dimensions for preoperative simulation and intraoperative navigation. The operation lasted 6 h and 42 min, and the blood loss volume was 30 mL. The patient's postoperative course was uneventful, and he was discharged on postoperative day 21.</p><p><strong>Conclusions: </strong>In a retrospective review of esophageal cancer surgery cases at our hospital, RTPV was observed in 17/314 cases (5.4%). The most common inflow site was the inferior pulmonary vein (IPV) (9 cases), followed by the left atrium (5 cases), superior pulmonary vein (2 cases), and superior branch of the IPV (1 case). The inflow site was behind the right main bronchus and the right intermediate bronchus in 4 and 13 cases, respectively. Compared to past reviews, the inflow site varied somewhat; however, the vascular location remained the same. By classifying the areas behind the right main and right intermediate bronchi as Zones 1 and 2, respectively, cases in which the RTPV runs through Zone 1, as identified on preoperative computed tomography, should be manipulated with caution due to the risk of injury during lymph node dissection beneath the tracheal bifurcation.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11873321/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.24-0093\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.24-0093","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/28 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
右上肺静脉(RTPV)是一种罕见的解剖变异,独立于右上肺叶出现。它在右主支气管或中间支气管后面流入左心房或另一条肺静脉。由于存在血管损伤的风险,这种异常给胸外科手术(如食管切除术)的隆下淋巴结清扫带来了挑战。RTPV主要位于右主支气管和右中间支气管后方;然而,缺乏针对这些部位的隆突下解剖的报道。在此,我们报告了一例食管癌伴RTPV的病例,该病例采用胸腔镜食管切除术治疗,并提出了一种方便的解剖结果和RTPV部位分类。病例介绍:一名71岁男性在常规体检期间接受了食管癌(T1bN0M0)的胸腔镜食管切除术。术前计算机断层扫描显示异常,RTPV在右主支气管后流入左心房。在保留RTPV的同时进行根治性隆突下淋巴结切除术,使用三维空间进行术前模拟和术中导航。手术时间6 h 42 min,出血量30 mL。患者术后过程平稳,于术后第21天出院。结论:回顾性分析我院食管癌手术病例,314例中有17例(5.4%)出现RTPV。最常见的流入部位为下肺静脉(IPV)(9例),其次为左心房(5例)、上肺静脉(2例)和上肺静脉分支(1例)。流入部位位于右主支气管后方4例,位于右中间支气管后方13例。与过去的评论相比,流入地点有所不同;然而,血管的位置保持不变。通过将右主支气管和右中间支气管后面的区域分别划分为1区和2区,术前计算机断层扫描发现RTPV穿过1区的病例应谨慎操作,因为在气管分叉下淋巴结清扫时存在损伤的风险。
Impact of Right Top Pulmonary Vein Location on Subcarinal Lymph Node Dissection in Thoracoscopic Esophagectomy: A Case Report and Literature Review.
Introduction: The right top pulmonary vein (RTPV) is a rare anatomical variant that arises independently of the right superior lobe. It drains behind the right main bronchus or bronchus intermedius and into the left atrium or another pulmonary vein. This anomaly poses challenges during subcarinal lymph node dissection in thoracic surgery, such as esophagectomy, owing to the risk of vascular injury. The RTPV is mainly located behind the right main bronchus and right intermediate bronchus; however, reports of subcarinal dissection focusing on these sites are lacking. Herein, we present a case of esophageal cancer with an RTPV that was treated with thoracoscopic esophagectomy and propose a convenient classification for the anatomical findings and RTPV site.
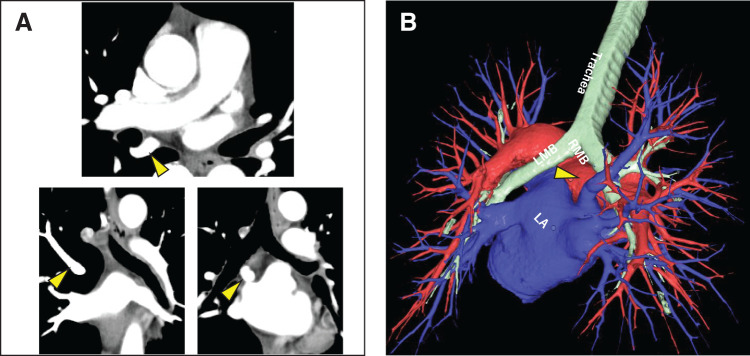
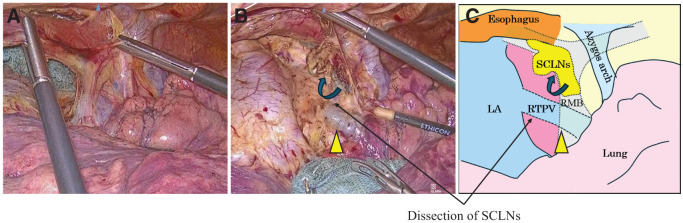
Case presentation: A 71-year-old man underwent a thoracoscopic esophagectomy for esophageal cancer (T1bN0M0) during a routine medical checkup. A preoperative computed tomography scan revealed an anomaly in which the RTPV drained into the left atrium behind the right main bronchus. Radical subcarinal lymphadenectomy was performed while preserving the RTPV, using 3 dimensions for preoperative simulation and intraoperative navigation. The operation lasted 6 h and 42 min, and the blood loss volume was 30 mL. The patient's postoperative course was uneventful, and he was discharged on postoperative day 21.
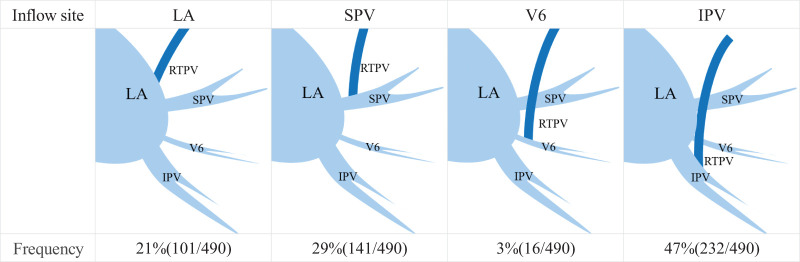
Conclusions: In a retrospective review of esophageal cancer surgery cases at our hospital, RTPV was observed in 17/314 cases (5.4%). The most common inflow site was the inferior pulmonary vein (IPV) (9 cases), followed by the left atrium (5 cases), superior pulmonary vein (2 cases), and superior branch of the IPV (1 case). The inflow site was behind the right main bronchus and the right intermediate bronchus in 4 and 13 cases, respectively. Compared to past reviews, the inflow site varied somewhat; however, the vascular location remained the same. By classifying the areas behind the right main and right intermediate bronchi as Zones 1 and 2, respectively, cases in which the RTPV runs through Zone 1, as identified on preoperative computed tomography, should be manipulated with caution due to the risk of injury during lymph node dissection beneath the tracheal bifurcation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


