Rajesh Kumar, Naveed Ullah Khan, Ali Bin Naseer, Zille Huma, Kalsoom Chachar, Maryam Samad, Muhammad Ishaq, Abiha Urooj, Uroosa Safdar, Muhammad Rasool, Sohail Khan, Jawaid Akbar Sial, Tahir Saghir, Nadeem Qamar
{"title":"收缩压与左室舒张末期压比与TIMI评分对经皮冠状动脉介入术后短期死亡率的预测准确性。","authors":"Rajesh Kumar, Naveed Ullah Khan, Ali Bin Naseer, Zille Huma, Kalsoom Chachar, Maryam Samad, Muhammad Ishaq, Abiha Urooj, Uroosa Safdar, Muhammad Rasool, Sohail Khan, Jawaid Akbar Sial, Tahir Saghir, Nadeem Qamar","doi":"10.34172/jcvtr.32933","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Aim of this study was to evaluate the predictive performance of systolic blood pressure (SBP) to left ventricular end-diastolic pressure (LVEDP) ratio for the prediction of in-hospital and short-term mortality in a contemporary cohort of patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) at a tertiary care cardiac center.</p><p><strong>Methods: </strong>This study included a consecutive series of patients diagnosed with STEMI who underwent primary PCI. The SBP/LVEDP ratio and TIMI (Thrombolysis in Myocardial Infarction) score were calculated, and their ability to predict in-hospital and short-term mortality was evaluated by analyzing the area under the curve (AUC) on the receiver operating characteristics (ROC) curve.</p><p><strong>Results: </strong>This study involved 977 patients, with 780 (79.8%) being male and a mean age of 55.6±11.5 years. Among them, 191 (19.5%) had an SBP/LVEDP≤5.4. The in-hospital mortality rate was 4.3% (42), and the short-term all-cause mortality rate after a mean follow-up of 5.9±2.4 months was 15% (140). Patients with SBP/LVEDP≤5.4 had higher in-hospital mortality rates (14.1% vs. 1.9%; <i>P</i><0.001) and short-term mortality rates (35.1% vs. 9.8%; <i>P</i><0.001) compared to those with SBP/LVEDP>5.4. The AUCs of SBP/LVEDP and TIMI for predicting in-hospital mortality were 0.766 [0.681-0.851] and 0.787 [0.713-0.861], respectively. For short-term mortality, the AUCs of SBP/LVEDP and TIMI were 0.731 [0.682-0.780] and 0.736 [0.690-0.782], respectively.</p><p><strong>Conclusion: </strong>In conclusion, SBP/LVEDP showed sufficiently high predictive power comparable to the TIMI risk score. SBP/LVEDP is a readily available ratio that can rapidly provide valuable prognostic information during primary PCI.</p>","PeriodicalId":15207,"journal":{"name":"Journal of Cardiovascular and Thoracic Research","volume":"16 4","pages":"235-242"},"PeriodicalIF":0.7000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11866769/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictive accuracy of systolic blood pressure to left ventricular end-diastolic pressure ratio versus TIMI score for short-term mortality after primary percutaneous coronary intervention.\",\"authors\":\"Rajesh Kumar, Naveed Ullah Khan, Ali Bin Naseer, Zille Huma, Kalsoom Chachar, Maryam Samad, Muhammad Ishaq, Abiha Urooj, Uroosa Safdar, Muhammad Rasool, Sohail Khan, Jawaid Akbar Sial, Tahir Saghir, Nadeem Qamar\",\"doi\":\"10.34172/jcvtr.32933\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Aim of this study was to evaluate the predictive performance of systolic blood pressure (SBP) to left ventricular end-diastolic pressure (LVEDP) ratio for the prediction of in-hospital and short-term mortality in a contemporary cohort of patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) at a tertiary care cardiac center.</p><p><strong>Methods: </strong>This study included a consecutive series of patients diagnosed with STEMI who underwent primary PCI. The SBP/LVEDP ratio and TIMI (Thrombolysis in Myocardial Infarction) score were calculated, and their ability to predict in-hospital and short-term mortality was evaluated by analyzing the area under the curve (AUC) on the receiver operating characteristics (ROC) curve.</p><p><strong>Results: </strong>This study involved 977 patients, with 780 (79.8%) being male and a mean age of 55.6±11.5 years. Among them, 191 (19.5%) had an SBP/LVEDP≤5.4. The in-hospital mortality rate was 4.3% (42), and the short-term all-cause mortality rate after a mean follow-up of 5.9±2.4 months was 15% (140). Patients with SBP/LVEDP≤5.4 had higher in-hospital mortality rates (14.1% vs. 1.9%; <i>P</i><0.001) and short-term mortality rates (35.1% vs. 9.8%; <i>P</i><0.001) compared to those with SBP/LVEDP>5.4. The AUCs of SBP/LVEDP and TIMI for predicting in-hospital mortality were 0.766 [0.681-0.851] and 0.787 [0.713-0.861], respectively. For short-term mortality, the AUCs of SBP/LVEDP and TIMI were 0.731 [0.682-0.780] and 0.736 [0.690-0.782], respectively.</p><p><strong>Conclusion: </strong>In conclusion, SBP/LVEDP showed sufficiently high predictive power comparable to the TIMI risk score. SBP/LVEDP is a readily available ratio that can rapidly provide valuable prognostic information during primary PCI.</p>\",\"PeriodicalId\":15207,\"journal\":{\"name\":\"Journal of Cardiovascular and Thoracic Research\",\"volume\":\"16 4\",\"pages\":\"235-242\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11866769/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular and Thoracic Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.34172/jcvtr.32933\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular and Thoracic Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34172/jcvtr.32933","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
简介:本研究的目的是评估收缩压(SBP)与左室舒张末期压(LVEDP)比对在三级保健心脏中心接受初级经皮冠状动脉介入治疗(PCI)的st段抬高型心肌梗死(STEMI)患者的住院和短期死亡率的预测性能。方法:本研究纳入了一系列被诊断为STEMI并接受首次PCI治疗的连续患者。计算SBP/LVEDP比值和TIMI (Thrombolysis in Myocardial Infarction,心肌梗死溶栓)评分,通过分析受试者工作特征(ROC)曲线下面积(AUC)评价其预测住院死亡率和短期死亡率的能力。结果:本研究纳入977例患者,其中780例(79.8%)为男性,平均年龄55.6±11.5岁。其中191例(19.5%)患者SBP/LVEDP≤5.4。住院死亡率4.3%(42人),平均随访5.9±2.4个月,短期全因死亡率15%(140人)。SBP/LVEDP≤5.4的患者住院死亡率更高(14.1% vs. 1.9%;PP5.4。SBP/LVEDP和TIMI预测住院死亡率的auc分别为0.766[0.681-0.851]和0.787[0.713-0.861]。短期死亡率方面,SBP/LVEDP和TIMI的auc分别为0.731[0.682-0.780]和0.736[0.690-0.782]。结论:与TIMI风险评分相比,SBP/LVEDP具有足够高的预测能力。收缩压/LVEDP是一个容易获得的比值,可以快速提供初步PCI治疗期间有价值的预后信息。
Predictive accuracy of systolic blood pressure to left ventricular end-diastolic pressure ratio versus TIMI score for short-term mortality after primary percutaneous coronary intervention.
Introduction: Aim of this study was to evaluate the predictive performance of systolic blood pressure (SBP) to left ventricular end-diastolic pressure (LVEDP) ratio for the prediction of in-hospital and short-term mortality in a contemporary cohort of patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) at a tertiary care cardiac center.
Methods: This study included a consecutive series of patients diagnosed with STEMI who underwent primary PCI. The SBP/LVEDP ratio and TIMI (Thrombolysis in Myocardial Infarction) score were calculated, and their ability to predict in-hospital and short-term mortality was evaluated by analyzing the area under the curve (AUC) on the receiver operating characteristics (ROC) curve.
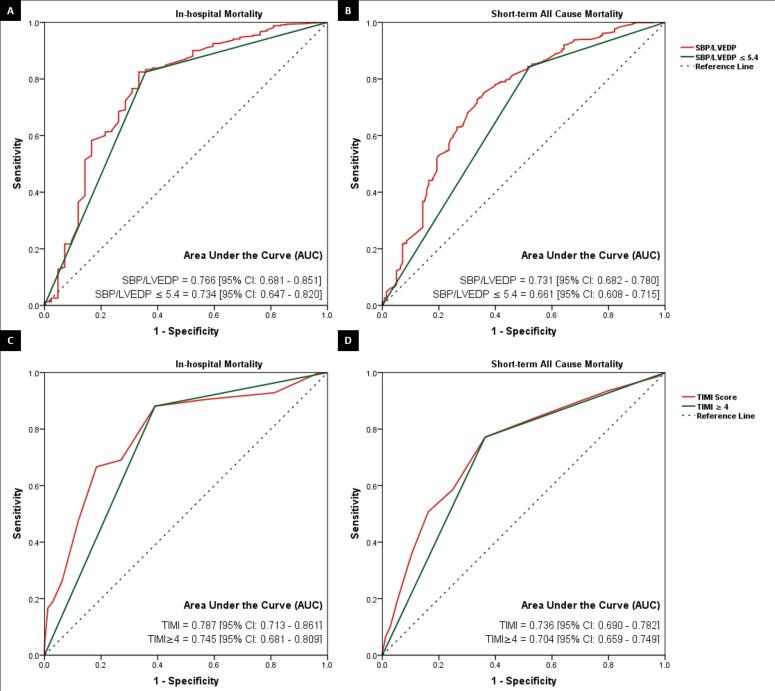
Results: This study involved 977 patients, with 780 (79.8%) being male and a mean age of 55.6±11.5 years. Among them, 191 (19.5%) had an SBP/LVEDP≤5.4. The in-hospital mortality rate was 4.3% (42), and the short-term all-cause mortality rate after a mean follow-up of 5.9±2.4 months was 15% (140). Patients with SBP/LVEDP≤5.4 had higher in-hospital mortality rates (14.1% vs. 1.9%; P<0.001) and short-term mortality rates (35.1% vs. 9.8%; P<0.001) compared to those with SBP/LVEDP>5.4. The AUCs of SBP/LVEDP and TIMI for predicting in-hospital mortality were 0.766 [0.681-0.851] and 0.787 [0.713-0.861], respectively. For short-term mortality, the AUCs of SBP/LVEDP and TIMI were 0.731 [0.682-0.780] and 0.736 [0.690-0.782], respectively.
Conclusion: In conclusion, SBP/LVEDP showed sufficiently high predictive power comparable to the TIMI risk score. SBP/LVEDP is a readily available ratio that can rapidly provide valuable prognostic information during primary PCI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


