ChaoPing Wu, Arif Canakoglu, Jacob Vine, Anya Mathur, Ronit Nath, Markos Kashiouris, Piyush Mathur, Ari Ercole, Paul Elbers, Abhijit Duggal, Ken Koon Wong, Anirban Bhattacharyya
{"title":"阐明机械动力与肺损伤的因果关系:呼吸机管理的动态方法。","authors":"ChaoPing Wu, Arif Canakoglu, Jacob Vine, Anya Mathur, Ronit Nath, Markos Kashiouris, Piyush Mathur, Ari Ercole, Paul Elbers, Abhijit Duggal, Ken Koon Wong, Anirban Bhattacharyya","doi":"10.1186/s40635-025-00736-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mechanical power (MP) serves as a crucial predictive indicator for ventilator-induced lung injury and plays a pivotal role in tailoring the management of mechanical ventilation. However, its application across different diseases and stages remains nuanced.</p><p><strong>Methods: </strong>Using AmsterdamUMCdb, we conducted a retrospective study to analyze the causal relationship between MP and outcomes of invasive mechanical ventilation, specifically SpO<sub>2</sub>/FiO<sub>2</sub> ratio (P/F) and ventilator-free days at day 28 (VFD28). We employed causal inferential analysis with backdoor linear regression and double machine learning, guided by directed acyclic graphs, to estimate the average treatment effect (ATE) in the whole population and conditional average treatment effect (CATE) in the individual cohort. Additionally, to enhance interpretability and identify MP thresholds, we conducted a simulation analysis.</p><p><strong>Results: </strong>In the study, we included 11,110 unique admissions into analysis, of which 58.3% (6391) were surgical admissions. We revealed a negative and significant causal effect of median MP on VFD28, with estimated ATEs of -0.135 (95% confidence interval [CI]: -0.15 to -0.121). The similar effect was not observed in Maximal MP and minimal MP. The effect of MP was more pronounced in the medical subgroup, with a CATE of -0.173 (95% CI: -0.197 to -0.143) determined through backdoor linear regression. Patients with cardio, respiratory, and infection diagnoses, who required long-term intubation, sustained higher impact on CATEs across various admission diagnoses. Our simulations showed that there is no single MP threshold that can be applied to all patients, as the optimal threshold varies depending on the patient's condition.</p><p><strong>Conclusion: </strong>Our study underscores the importance of tailoring MP adjustments on an individualized basis in ventilator management. This approach opens up new avenues for personalized treatment strategies and provides fresh insights into the real-time impact of MP in diverse clinical scenarios. It highlights the significance of median MP while acknowledging the absence of universally applicable thresholds.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"28"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11871266/pdf/","citationCount":"0","resultStr":"{\"title\":\"Elucidating the causal relationship of mechanical power and lung injury: a dynamic approach to ventilator management.\",\"authors\":\"ChaoPing Wu, Arif Canakoglu, Jacob Vine, Anya Mathur, Ronit Nath, Markos Kashiouris, Piyush Mathur, Ari Ercole, Paul Elbers, Abhijit Duggal, Ken Koon Wong, Anirban Bhattacharyya\",\"doi\":\"10.1186/s40635-025-00736-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Mechanical power (MP) serves as a crucial predictive indicator for ventilator-induced lung injury and plays a pivotal role in tailoring the management of mechanical ventilation. However, its application across different diseases and stages remains nuanced.</p><p><strong>Methods: </strong>Using AmsterdamUMCdb, we conducted a retrospective study to analyze the causal relationship between MP and outcomes of invasive mechanical ventilation, specifically SpO<sub>2</sub>/FiO<sub>2</sub> ratio (P/F) and ventilator-free days at day 28 (VFD28). We employed causal inferential analysis with backdoor linear regression and double machine learning, guided by directed acyclic graphs, to estimate the average treatment effect (ATE) in the whole population and conditional average treatment effect (CATE) in the individual cohort. Additionally, to enhance interpretability and identify MP thresholds, we conducted a simulation analysis.</p><p><strong>Results: </strong>In the study, we included 11,110 unique admissions into analysis, of which 58.3% (6391) were surgical admissions. We revealed a negative and significant causal effect of median MP on VFD28, with estimated ATEs of -0.135 (95% confidence interval [CI]: -0.15 to -0.121). The similar effect was not observed in Maximal MP and minimal MP. The effect of MP was more pronounced in the medical subgroup, with a CATE of -0.173 (95% CI: -0.197 to -0.143) determined through backdoor linear regression. Patients with cardio, respiratory, and infection diagnoses, who required long-term intubation, sustained higher impact on CATEs across various admission diagnoses. Our simulations showed that there is no single MP threshold that can be applied to all patients, as the optimal threshold varies depending on the patient's condition.</p><p><strong>Conclusion: </strong>Our study underscores the importance of tailoring MP adjustments on an individualized basis in ventilator management. This approach opens up new avenues for personalized treatment strategies and provides fresh insights into the real-time impact of MP in diverse clinical scenarios. It highlights the significance of median MP while acknowledging the absence of universally applicable thresholds.</p>\",\"PeriodicalId\":13750,\"journal\":{\"name\":\"Intensive Care Medicine Experimental\",\"volume\":\"13 1\",\"pages\":\"28\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-02-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11871266/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Intensive Care Medicine Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40635-025-00736-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00736-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Elucidating the causal relationship of mechanical power and lung injury: a dynamic approach to ventilator management.
Background: Mechanical power (MP) serves as a crucial predictive indicator for ventilator-induced lung injury and plays a pivotal role in tailoring the management of mechanical ventilation. However, its application across different diseases and stages remains nuanced.
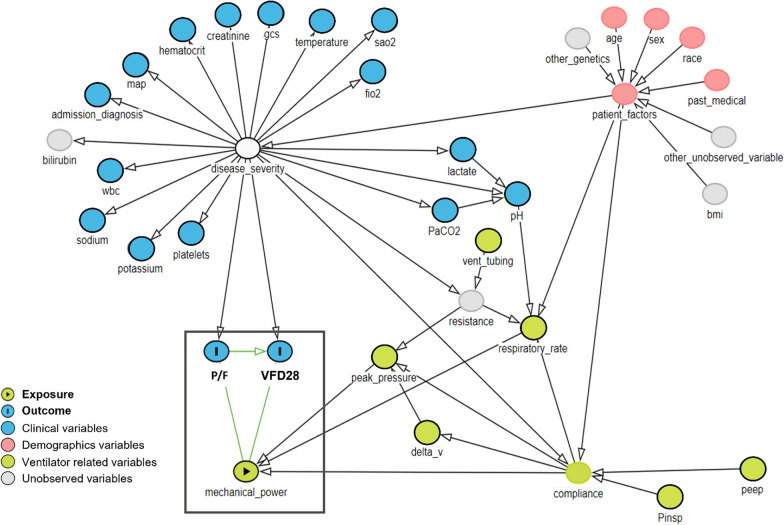
Methods: Using AmsterdamUMCdb, we conducted a retrospective study to analyze the causal relationship between MP and outcomes of invasive mechanical ventilation, specifically SpO2/FiO2 ratio (P/F) and ventilator-free days at day 28 (VFD28). We employed causal inferential analysis with backdoor linear regression and double machine learning, guided by directed acyclic graphs, to estimate the average treatment effect (ATE) in the whole population and conditional average treatment effect (CATE) in the individual cohort. Additionally, to enhance interpretability and identify MP thresholds, we conducted a simulation analysis.
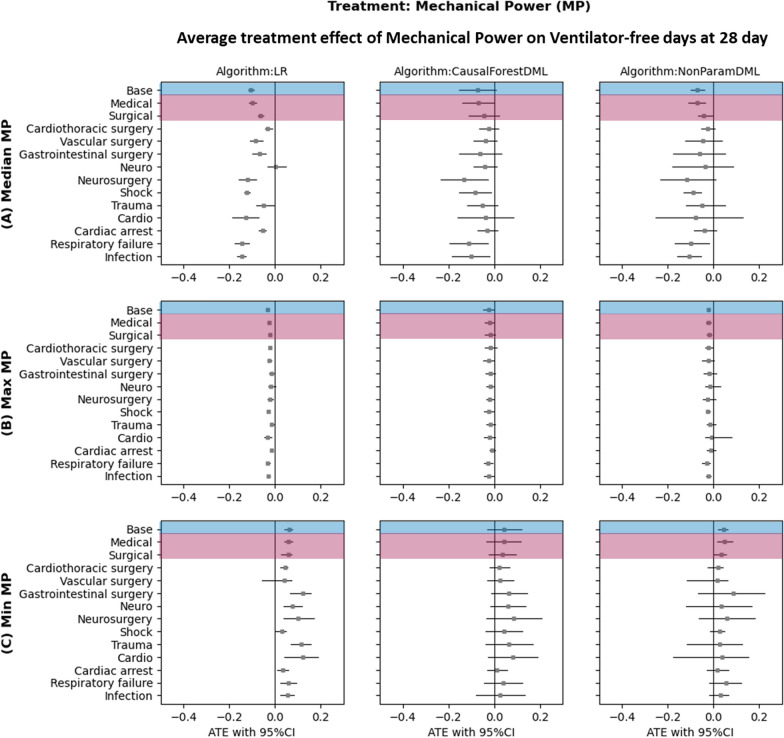
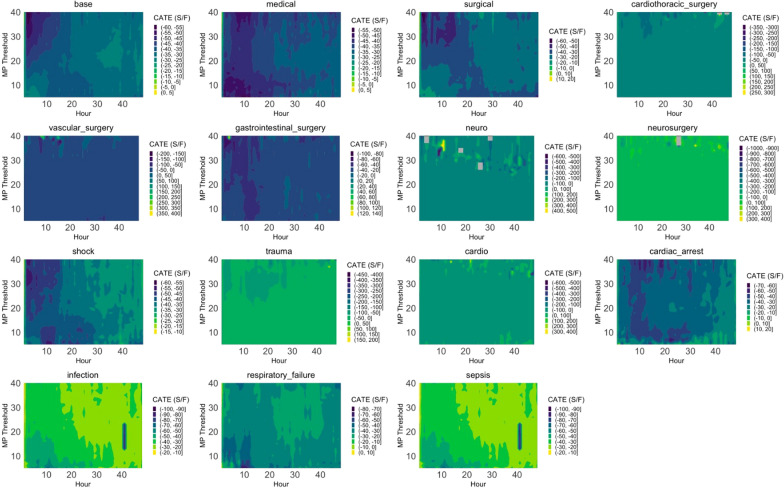
Results: In the study, we included 11,110 unique admissions into analysis, of which 58.3% (6391) were surgical admissions. We revealed a negative and significant causal effect of median MP on VFD28, with estimated ATEs of -0.135 (95% confidence interval [CI]: -0.15 to -0.121). The similar effect was not observed in Maximal MP and minimal MP. The effect of MP was more pronounced in the medical subgroup, with a CATE of -0.173 (95% CI: -0.197 to -0.143) determined through backdoor linear regression. Patients with cardio, respiratory, and infection diagnoses, who required long-term intubation, sustained higher impact on CATEs across various admission diagnoses. Our simulations showed that there is no single MP threshold that can be applied to all patients, as the optimal threshold varies depending on the patient's condition.
Conclusion: Our study underscores the importance of tailoring MP adjustments on an individualized basis in ventilator management. This approach opens up new avenues for personalized treatment strategies and provides fresh insights into the real-time impact of MP in diverse clinical scenarios. It highlights the significance of median MP while acknowledging the absence of universally applicable thresholds.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


