Benjamin Clay, Balamrit S Sokhal, Sarah Zeriouh, Neil T Srinivasan, Parag R Gajendragadkar, Claire A Martin
{"title":"温度控制消融与常规消融肺静脉隔离治疗房颤:系统回顾和荟萃分析。","authors":"Benjamin Clay, Balamrit S Sokhal, Sarah Zeriouh, Neil T Srinivasan, Parag R Gajendragadkar, Claire A Martin","doi":"10.15420/aer.2024.41","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study compared the efficacy and safety of temperature-controlled and conventional contact-force-sensing radiofrequency ablation catheters for pulmonary vein isolation (PVI) in AF.</p><p><strong>Methods: </strong>Seven studies (1,138 patients) were included. Randomised controlled trials and observational (single-arm and two-arm) studies that reported freedom from AF ≥3 months after PVI with temperature-controlled radiofrequency ablation catheters (Biosense Webster QDOT MICRO operating in QMODE or Medtronic DiamondTemp) were included.</p><p><strong>Results: </strong>Freedom from AF at a mean (± SD) follow-up of 9.0 ± 3.6 months did not differ significantly between temperature-controlled and conventional ablation (OR 1.22; 95% CI [-0.79, 1.64]; p=0.24). Total procedure duration (-13.5 minutes; 95% CI [-17.1, -10.0 minutes]; p<0.001) and total ablation duration (-8.9 min; 95% CI [-10.3, -7.5 min]; p<0.01) were significantly shorter for temperature-controlled ablation. There were no significant differences between temperature-controlled and conventional ablation in either the aggregated rates of procedural complications (OR 0.69; 95% CI [-0.15, 1.54]; p=0.11) or in the rate of any individual complication.</p><p><strong>Conclusion: </strong>Temperature-controlled ablation was found to be at least non-inferior to conventional ablation in all measures of efficacy and safety. Further randomised controlled trials are warranted to evaluate long-term rates of freedom from AF and patient comfort.</p>","PeriodicalId":8412,"journal":{"name":"Arrhythmia & Electrophysiology Review","volume":"14 ","pages":"e03"},"PeriodicalIF":3.3000,"publicationDate":"2025-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11865669/pdf/","citationCount":"0","resultStr":"{\"title\":\"Temperature-controlled Ablation Versus Conventional Ablation for Pulmonary Vein Isolation in the Treatment of AF: A Systematic Review and Meta-Analysis.\",\"authors\":\"Benjamin Clay, Balamrit S Sokhal, Sarah Zeriouh, Neil T Srinivasan, Parag R Gajendragadkar, Claire A Martin\",\"doi\":\"10.15420/aer.2024.41\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study compared the efficacy and safety of temperature-controlled and conventional contact-force-sensing radiofrequency ablation catheters for pulmonary vein isolation (PVI) in AF.</p><p><strong>Methods: </strong>Seven studies (1,138 patients) were included. Randomised controlled trials and observational (single-arm and two-arm) studies that reported freedom from AF ≥3 months after PVI with temperature-controlled radiofrequency ablation catheters (Biosense Webster QDOT MICRO operating in QMODE or Medtronic DiamondTemp) were included.</p><p><strong>Results: </strong>Freedom from AF at a mean (± SD) follow-up of 9.0 ± 3.6 months did not differ significantly between temperature-controlled and conventional ablation (OR 1.22; 95% CI [-0.79, 1.64]; p=0.24). Total procedure duration (-13.5 minutes; 95% CI [-17.1, -10.0 minutes]; p<0.001) and total ablation duration (-8.9 min; 95% CI [-10.3, -7.5 min]; p<0.01) were significantly shorter for temperature-controlled ablation. There were no significant differences between temperature-controlled and conventional ablation in either the aggregated rates of procedural complications (OR 0.69; 95% CI [-0.15, 1.54]; p=0.11) or in the rate of any individual complication.</p><p><strong>Conclusion: </strong>Temperature-controlled ablation was found to be at least non-inferior to conventional ablation in all measures of efficacy and safety. Further randomised controlled trials are warranted to evaluate long-term rates of freedom from AF and patient comfort.</p>\",\"PeriodicalId\":8412,\"journal\":{\"name\":\"Arrhythmia & Electrophysiology Review\",\"volume\":\"14 \",\"pages\":\"e03\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-01-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11865669/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arrhythmia & Electrophysiology Review\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15420/aer.2024.41\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arrhythmia & Electrophysiology Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/aer.2024.41","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Temperature-controlled Ablation Versus Conventional Ablation for Pulmonary Vein Isolation in the Treatment of AF: A Systematic Review and Meta-Analysis.
Background: This study compared the efficacy and safety of temperature-controlled and conventional contact-force-sensing radiofrequency ablation catheters for pulmonary vein isolation (PVI) in AF.
Methods: Seven studies (1,138 patients) were included. Randomised controlled trials and observational (single-arm and two-arm) studies that reported freedom from AF ≥3 months after PVI with temperature-controlled radiofrequency ablation catheters (Biosense Webster QDOT MICRO operating in QMODE or Medtronic DiamondTemp) were included.
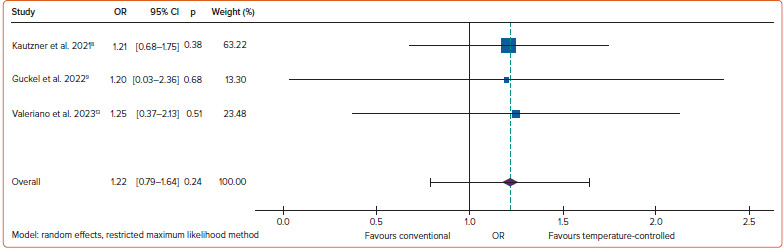
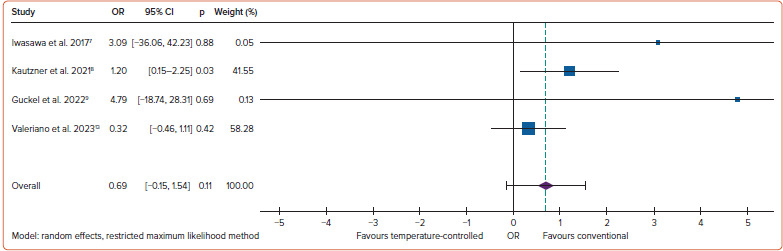
Results: Freedom from AF at a mean (± SD) follow-up of 9.0 ± 3.6 months did not differ significantly between temperature-controlled and conventional ablation (OR 1.22; 95% CI [-0.79, 1.64]; p=0.24). Total procedure duration (-13.5 minutes; 95% CI [-17.1, -10.0 minutes]; p<0.001) and total ablation duration (-8.9 min; 95% CI [-10.3, -7.5 min]; p<0.01) were significantly shorter for temperature-controlled ablation. There were no significant differences between temperature-controlled and conventional ablation in either the aggregated rates of procedural complications (OR 0.69; 95% CI [-0.15, 1.54]; p=0.11) or in the rate of any individual complication.
Conclusion: Temperature-controlled ablation was found to be at least non-inferior to conventional ablation in all measures of efficacy and safety. Further randomised controlled trials are warranted to evaluate long-term rates of freedom from AF and patient comfort.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


