{"title":"严重登革、动脉瘤性蛛网膜下腔出血及噬血细胞性淋巴组织细胞增多症:罕见合并病例。","authors":"Saboor Mateen, Ajay Mishra, Shivesh Singh, Firdaus Jabeen","doi":"10.31744/einstein_journal/2025RC1209","DOIUrl":null,"url":null,"abstract":"<p><p>Dengue, a vector-borne acute febrile illness caused by members of the Flavivirus genus, has dramatically increased its occurrence worldwide. Neurological complications of dengue range from 2.63 to 40%, and subarachnoid hemorrhage is a rare, but significant manifestation. Hemophagocytic lymphohistiocytosis is a life-threatening hyperinflammatory syndrome, sometimes secondary to infections such as dengue. This report presents a rare case of severe dengue with subarachnoid hemorrhage and hemophagocytic lymphohistiocytosis. A 19-year-old male presented with a 7-day history of fever and myalgia, followed by severe headache and vomiting. Initial examination revealed high fever, hepatosplenomegaly, and pancytopenia. Lumbar puncture confirmed via computed tomography showed a Fisher Grade 2 subarachnoid hemorrhage with a small aneurysm at the junction of the left anterior coronary and anterior communicating arteries. Secondary hemophagocytic lymphohistiocytosis was diagnosed based on the criteria from 2004, with elevated inflammatory markers, hypertriglyceridemia, and hyperferritinemia. The patient was treated conservatively with intravenous fluids, osmotic diuretics, antiepileptics, steroids, and nimodipine. The patient showed clinical improvement and was discharged on the 11th day. Isolated subarachnoid hemorrhage is rare in dengue. The hyperinflammatory state in hemophagocytic lymphohistiocytosis, which is often overlooked due to nonspecific symptoms, can lead to aneurysm formation and rupture. Persistent fever, cytopenia, and hyperferritinemia should raise suspicion of hemophagocytic lymphohistiocytosis in cases of severe dengue with neurological complications. In patients with severe dengue and intracranial hemorrhage, clinicians should remain cautious for hemophagocytic lymphohistiocytosis to reduce the associated morbidity and mortality.</p>","PeriodicalId":47359,"journal":{"name":"Einstein-Sao Paulo","volume":"23 ","pages":"eRC1209"},"PeriodicalIF":0.9000,"publicationDate":"2025-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11869786/pdf/","citationCount":"0","resultStr":"{\"title\":\"Severe dengue, aneurysmal sub-arachnoid hemorrhage, and hemophagocytic lymphohistiocytosis: a rare case combination.\",\"authors\":\"Saboor Mateen, Ajay Mishra, Shivesh Singh, Firdaus Jabeen\",\"doi\":\"10.31744/einstein_journal/2025RC1209\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Dengue, a vector-borne acute febrile illness caused by members of the Flavivirus genus, has dramatically increased its occurrence worldwide. Neurological complications of dengue range from 2.63 to 40%, and subarachnoid hemorrhage is a rare, but significant manifestation. Hemophagocytic lymphohistiocytosis is a life-threatening hyperinflammatory syndrome, sometimes secondary to infections such as dengue. This report presents a rare case of severe dengue with subarachnoid hemorrhage and hemophagocytic lymphohistiocytosis. A 19-year-old male presented with a 7-day history of fever and myalgia, followed by severe headache and vomiting. Initial examination revealed high fever, hepatosplenomegaly, and pancytopenia. Lumbar puncture confirmed via computed tomography showed a Fisher Grade 2 subarachnoid hemorrhage with a small aneurysm at the junction of the left anterior coronary and anterior communicating arteries. Secondary hemophagocytic lymphohistiocytosis was diagnosed based on the criteria from 2004, with elevated inflammatory markers, hypertriglyceridemia, and hyperferritinemia. The patient was treated conservatively with intravenous fluids, osmotic diuretics, antiepileptics, steroids, and nimodipine. The patient showed clinical improvement and was discharged on the 11th day. Isolated subarachnoid hemorrhage is rare in dengue. The hyperinflammatory state in hemophagocytic lymphohistiocytosis, which is often overlooked due to nonspecific symptoms, can lead to aneurysm formation and rupture. Persistent fever, cytopenia, and hyperferritinemia should raise suspicion of hemophagocytic lymphohistiocytosis in cases of severe dengue with neurological complications. In patients with severe dengue and intracranial hemorrhage, clinicians should remain cautious for hemophagocytic lymphohistiocytosis to reduce the associated morbidity and mortality.</p>\",\"PeriodicalId\":47359,\"journal\":{\"name\":\"Einstein-Sao Paulo\",\"volume\":\"23 \",\"pages\":\"eRC1209\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-02-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11869786/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Einstein-Sao Paulo\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31744/einstein_journal/2025RC1209\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Einstein-Sao Paulo","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31744/einstein_journal/2025RC1209","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Severe dengue, aneurysmal sub-arachnoid hemorrhage, and hemophagocytic lymphohistiocytosis: a rare case combination.
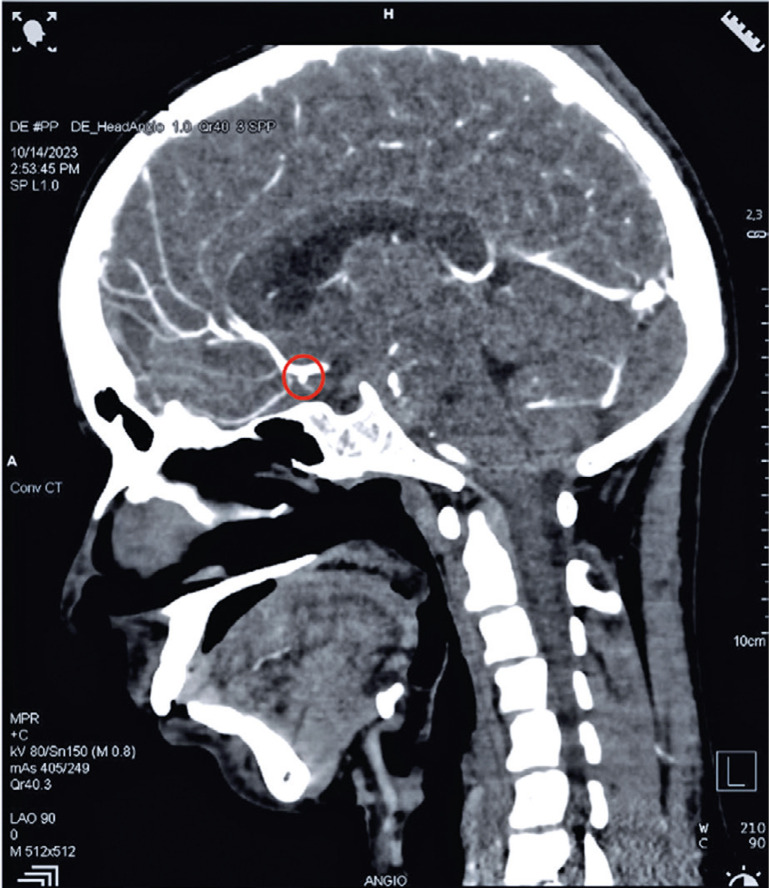
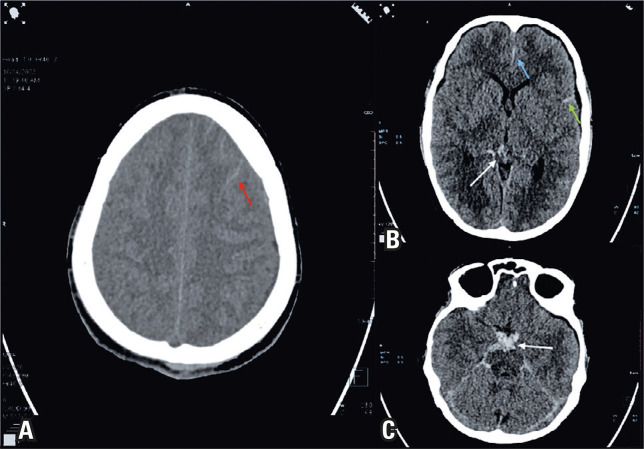
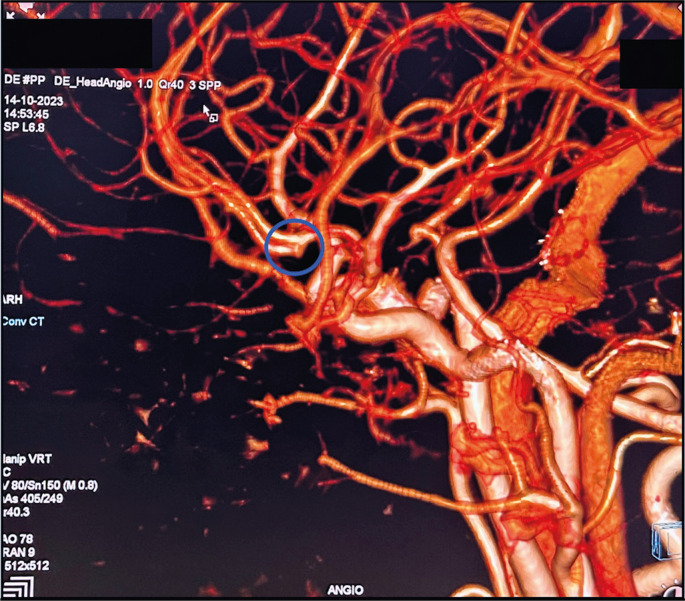
Dengue, a vector-borne acute febrile illness caused by members of the Flavivirus genus, has dramatically increased its occurrence worldwide. Neurological complications of dengue range from 2.63 to 40%, and subarachnoid hemorrhage is a rare, but significant manifestation. Hemophagocytic lymphohistiocytosis is a life-threatening hyperinflammatory syndrome, sometimes secondary to infections such as dengue. This report presents a rare case of severe dengue with subarachnoid hemorrhage and hemophagocytic lymphohistiocytosis. A 19-year-old male presented with a 7-day history of fever and myalgia, followed by severe headache and vomiting. Initial examination revealed high fever, hepatosplenomegaly, and pancytopenia. Lumbar puncture confirmed via computed tomography showed a Fisher Grade 2 subarachnoid hemorrhage with a small aneurysm at the junction of the left anterior coronary and anterior communicating arteries. Secondary hemophagocytic lymphohistiocytosis was diagnosed based on the criteria from 2004, with elevated inflammatory markers, hypertriglyceridemia, and hyperferritinemia. The patient was treated conservatively with intravenous fluids, osmotic diuretics, antiepileptics, steroids, and nimodipine. The patient showed clinical improvement and was discharged on the 11th day. Isolated subarachnoid hemorrhage is rare in dengue. The hyperinflammatory state in hemophagocytic lymphohistiocytosis, which is often overlooked due to nonspecific symptoms, can lead to aneurysm formation and rupture. Persistent fever, cytopenia, and hyperferritinemia should raise suspicion of hemophagocytic lymphohistiocytosis in cases of severe dengue with neurological complications. In patients with severe dengue and intracranial hemorrhage, clinicians should remain cautious for hemophagocytic lymphohistiocytosis to reduce the associated morbidity and mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


