{"title":"在 MIMIC IV 数据库中,高钾血症与重症患者的短期和中期死亡率有关。","authors":"Chuan Xu, Yong Luo, Xiuling Chen, Yunlin Feng","doi":"10.1038/s41598-025-91194-7","DOIUrl":null,"url":null,"abstract":"<p><p>We aimed to explore the association of hyperkalemia and short- and mid-term mortality in critically ill patients using the Medical Information Mart for Intensive Care (MIMIC-IV) database. Adult patients who had been stayed in the intensive care unit (ICU) for at least 48 h and tested for serum potassium were included. Hyperkalemia was defined as serum potassium higher than 5.5 mmol/L. Exposures included the occurrence the timing of hyperkalemia and the numeric values of serum potassium. The outcomes included ICU mortality and 7 days and 30 days mortality after ICU admission. Survival curves were calculated according to Kaplan-Meier analysis. Univariate and multivariate Cox proportional hazard regression models were used to estimate the hazard ratio (HR) and 95% confidence interval (CI) of each exposure for the outcomes. Subgroup analyses after full adjustment were conducted. A total of 22,370 ICU patients were included in this study. The prevalence of hyperkalemia was 18.8%. Patients with and without hyperkalemia differed significantly in a number of baseline characteristics. The ICU mortality, 7 days mortality, and 30 days mortality rates in the overall population were 12.6%, 9.5%, and 19.1%, respectively. After full adjustment, the occurrence of hyperkalemia is closely associated with the ICU mortality (HR: 1.39; 95% CI: 1.22-1.58) and 30 days mortality (HR: 1.16; 95% CI: 1.03-1.31) of the ICU patients. The timing of hyperkalemia is also associated with the risk of mortalities. These associations remained unchanged in the multiple regression analysis after full adjustment for the demographic variables, clinical tests, and comorbidities. In conclusion, the occurrence and timing of hyperkalemia are closely associated with the ICU and 30 days mortalities of critically ill patients. Once hyperkalemia occurs, active interventions are needed to restore serum potassium levels, regardless of the numeric values, to normal as quickly as possible.</p>","PeriodicalId":21811,"journal":{"name":"Scientific Reports","volume":"15 1","pages":"6539"},"PeriodicalIF":3.9000,"publicationDate":"2025-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11850630/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hyperkalemia is associated with short- and mid-term mortalities in critically ill patients in the MIMIC IV database.\",\"authors\":\"Chuan Xu, Yong Luo, Xiuling Chen, Yunlin Feng\",\"doi\":\"10.1038/s41598-025-91194-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We aimed to explore the association of hyperkalemia and short- and mid-term mortality in critically ill patients using the Medical Information Mart for Intensive Care (MIMIC-IV) database. Adult patients who had been stayed in the intensive care unit (ICU) for at least 48 h and tested for serum potassium were included. Hyperkalemia was defined as serum potassium higher than 5.5 mmol/L. Exposures included the occurrence the timing of hyperkalemia and the numeric values of serum potassium. The outcomes included ICU mortality and 7 days and 30 days mortality after ICU admission. Survival curves were calculated according to Kaplan-Meier analysis. Univariate and multivariate Cox proportional hazard regression models were used to estimate the hazard ratio (HR) and 95% confidence interval (CI) of each exposure for the outcomes. Subgroup analyses after full adjustment were conducted. A total of 22,370 ICU patients were included in this study. The prevalence of hyperkalemia was 18.8%. Patients with and without hyperkalemia differed significantly in a number of baseline characteristics. The ICU mortality, 7 days mortality, and 30 days mortality rates in the overall population were 12.6%, 9.5%, and 19.1%, respectively. After full adjustment, the occurrence of hyperkalemia is closely associated with the ICU mortality (HR: 1.39; 95% CI: 1.22-1.58) and 30 days mortality (HR: 1.16; 95% CI: 1.03-1.31) of the ICU patients. The timing of hyperkalemia is also associated with the risk of mortalities. These associations remained unchanged in the multiple regression analysis after full adjustment for the demographic variables, clinical tests, and comorbidities. In conclusion, the occurrence and timing of hyperkalemia are closely associated with the ICU and 30 days mortalities of critically ill patients. Once hyperkalemia occurs, active interventions are needed to restore serum potassium levels, regardless of the numeric values, to normal as quickly as possible.</p>\",\"PeriodicalId\":21811,\"journal\":{\"name\":\"Scientific Reports\",\"volume\":\"15 1\",\"pages\":\"6539\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2025-02-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11850630/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scientific Reports\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1038/s41598-025-91194-7\",\"RegionNum\":2,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scientific Reports","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1038/s41598-025-91194-7","RegionNum":2,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Hyperkalemia is associated with short- and mid-term mortalities in critically ill patients in the MIMIC IV database.
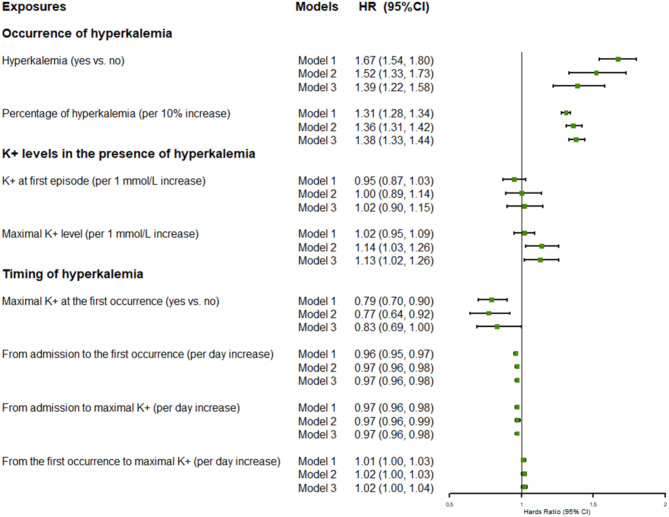
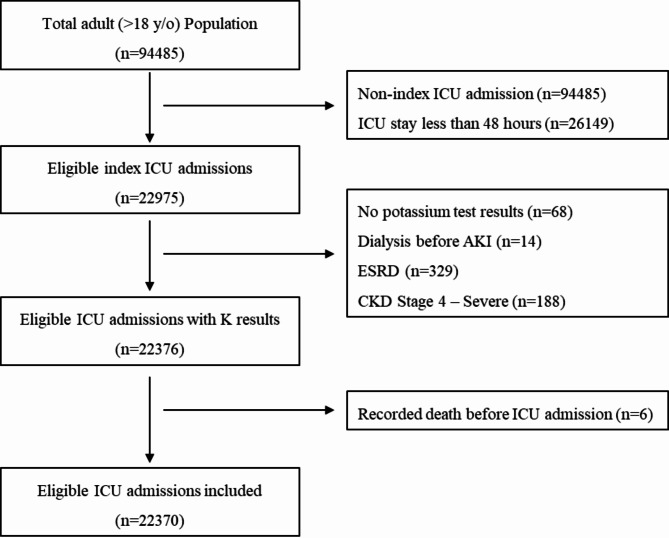
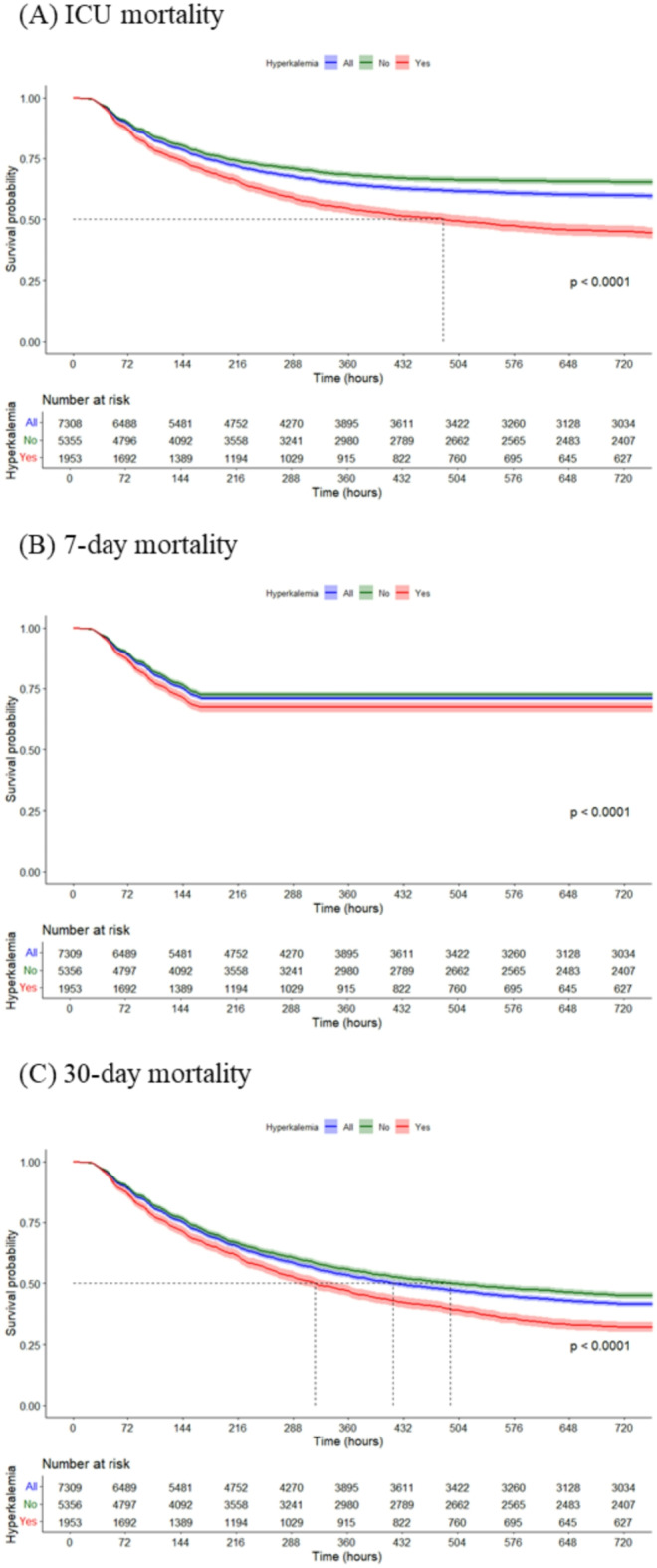
We aimed to explore the association of hyperkalemia and short- and mid-term mortality in critically ill patients using the Medical Information Mart for Intensive Care (MIMIC-IV) database. Adult patients who had been stayed in the intensive care unit (ICU) for at least 48 h and tested for serum potassium were included. Hyperkalemia was defined as serum potassium higher than 5.5 mmol/L. Exposures included the occurrence the timing of hyperkalemia and the numeric values of serum potassium. The outcomes included ICU mortality and 7 days and 30 days mortality after ICU admission. Survival curves were calculated according to Kaplan-Meier analysis. Univariate and multivariate Cox proportional hazard regression models were used to estimate the hazard ratio (HR) and 95% confidence interval (CI) of each exposure for the outcomes. Subgroup analyses after full adjustment were conducted. A total of 22,370 ICU patients were included in this study. The prevalence of hyperkalemia was 18.8%. Patients with and without hyperkalemia differed significantly in a number of baseline characteristics. The ICU mortality, 7 days mortality, and 30 days mortality rates in the overall population were 12.6%, 9.5%, and 19.1%, respectively. After full adjustment, the occurrence of hyperkalemia is closely associated with the ICU mortality (HR: 1.39; 95% CI: 1.22-1.58) and 30 days mortality (HR: 1.16; 95% CI: 1.03-1.31) of the ICU patients. The timing of hyperkalemia is also associated with the risk of mortalities. These associations remained unchanged in the multiple regression analysis after full adjustment for the demographic variables, clinical tests, and comorbidities. In conclusion, the occurrence and timing of hyperkalemia are closely associated with the ICU and 30 days mortalities of critically ill patients. Once hyperkalemia occurs, active interventions are needed to restore serum potassium levels, regardless of the numeric values, to normal as quickly as possible.
期刊介绍:
We publish original research from all areas of the natural sciences, psychology, medicine and engineering. You can learn more about what we publish by browsing our specific scientific subject areas below or explore Scientific Reports by browsing all articles and collections.
Scientific Reports has a 2-year impact factor: 4.380 (2021), and is the 6th most-cited journal in the world, with more than 540,000 citations in 2020 (Clarivate Analytics, 2021).
•Engineering
Engineering covers all aspects of engineering, technology, and applied science. It plays a crucial role in the development of technologies to address some of the world''s biggest challenges, helping to save lives and improve the way we live.
•Physical sciences
Physical sciences are those academic disciplines that aim to uncover the underlying laws of nature — often written in the language of mathematics. It is a collective term for areas of study including astronomy, chemistry, materials science and physics.
•Earth and environmental sciences
Earth and environmental sciences cover all aspects of Earth and planetary science and broadly encompass solid Earth processes, surface and atmospheric dynamics, Earth system history, climate and climate change, marine and freshwater systems, and ecology. It also considers the interactions between humans and these systems.
•Biological sciences
Biological sciences encompass all the divisions of natural sciences examining various aspects of vital processes. The concept includes anatomy, physiology, cell biology, biochemistry and biophysics, and covers all organisms from microorganisms, animals to plants.
•Health sciences
The health sciences study health, disease and healthcare. This field of study aims to develop knowledge, interventions and technology for use in healthcare to improve the treatment of patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


