John K Yue, Jun Yeop Oh, Alexander A Aabedi, Jia-Shu Chen, Kenneth X Probst, Vinil N Shah, Rosanna L Wustrack, Line G Jacques
{"title":"股骨环扎针穿透坐骨神经后的深度神经病变:说明病例和处理策略。","authors":"John K Yue, Jun Yeop Oh, Alexander A Aabedi, Jia-Shu Chen, Kenneth X Probst, Vinil N Shah, Rosanna L Wustrack, Line G Jacques","doi":"10.1089/neur.2024.0156","DOIUrl":null,"url":null,"abstract":"<p><p>Sciatic nerve injury associated with total hip arthroplasty (THA) confers chronic and progressive disability. Mechanisms of injury are heterogeneous and management nuances are often case-specific. We discuss a Sunderland Type 4 sciatic nerve transection by femoral cerclage wire from prior THA to highlight optimal clinical strategies when approaching complex cases. A 65-year-old woman presented to the neurosurgery clinic with worsening, medically refractory right sciatic sensorimotor neuropathy that began 1 year after ipsilateral hip arthroplasty. Neurological examination detected weakness in ankle dorsiflexion/plantarflexion and foot inversion/eversion (motor scale 2-3/5), toe extension/flexion (1/5), foot numbness, and hyperesthesia. Electromyogram confirmed sciatic neuropathy. Magnetic resonance neurogram (MRN) showed a thickened right sciatic nerve abutting a femoral cerclage wire, which appeared contiguous on reconstructed computed tomography imaging. Intraoperatively, the wire was discovered to have clearly transected and remained lodged within the sciatic nerve, requiring orthopedic surgery consultation and wire cutdown at the transection site. The surrounding neuroma was excised and the defect was reconstructed using nerve allograft interposition. Intraoperative neurophysiology monitoring (IONM) signals remained stable. Radiographs confirmed uncomplicated wire disconnection. The patient was discharged home the next day and reported significant symptomatic relief at 1-month follow-up. Delayed presentation of sciatic nerve transection by femoral cerclage wire with ongoing neural compression is rare. The anatomy of injury can be high risk, impelling thoughtful operative planning in THA as well as neuroplasty cases. Strategies include preoperative MRN to evaluate the pathoanatomy of nerve injury, neurosurgery and orthopedic surgery comanagement, and multimodal IONM to reduce risks of intraoperative neural injury and optimize outcomes.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"6 1","pages":"128-135"},"PeriodicalIF":1.8000,"publicationDate":"2025-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11839513/pdf/","citationCount":"0","resultStr":"{\"title\":\"Profound Neuropathy after Penetrating Transection of the Sciatic Nerve by Femoral Cerclage Wire: Illustrative Case and Management Strategy.\",\"authors\":\"John K Yue, Jun Yeop Oh, Alexander A Aabedi, Jia-Shu Chen, Kenneth X Probst, Vinil N Shah, Rosanna L Wustrack, Line G Jacques\",\"doi\":\"10.1089/neur.2024.0156\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Sciatic nerve injury associated with total hip arthroplasty (THA) confers chronic and progressive disability. Mechanisms of injury are heterogeneous and management nuances are often case-specific. We discuss a Sunderland Type 4 sciatic nerve transection by femoral cerclage wire from prior THA to highlight optimal clinical strategies when approaching complex cases. A 65-year-old woman presented to the neurosurgery clinic with worsening, medically refractory right sciatic sensorimotor neuropathy that began 1 year after ipsilateral hip arthroplasty. Neurological examination detected weakness in ankle dorsiflexion/plantarflexion and foot inversion/eversion (motor scale 2-3/5), toe extension/flexion (1/5), foot numbness, and hyperesthesia. Electromyogram confirmed sciatic neuropathy. Magnetic resonance neurogram (MRN) showed a thickened right sciatic nerve abutting a femoral cerclage wire, which appeared contiguous on reconstructed computed tomography imaging. Intraoperatively, the wire was discovered to have clearly transected and remained lodged within the sciatic nerve, requiring orthopedic surgery consultation and wire cutdown at the transection site. The surrounding neuroma was excised and the defect was reconstructed using nerve allograft interposition. Intraoperative neurophysiology monitoring (IONM) signals remained stable. Radiographs confirmed uncomplicated wire disconnection. The patient was discharged home the next day and reported significant symptomatic relief at 1-month follow-up. Delayed presentation of sciatic nerve transection by femoral cerclage wire with ongoing neural compression is rare. The anatomy of injury can be high risk, impelling thoughtful operative planning in THA as well as neuroplasty cases. Strategies include preoperative MRN to evaluate the pathoanatomy of nerve injury, neurosurgery and orthopedic surgery comanagement, and multimodal IONM to reduce risks of intraoperative neural injury and optimize outcomes.</p>\",\"PeriodicalId\":74300,\"journal\":{\"name\":\"Neurotrauma reports\",\"volume\":\"6 1\",\"pages\":\"128-135\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-01-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11839513/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurotrauma reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/neur.2024.0156\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2024.0156","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Profound Neuropathy after Penetrating Transection of the Sciatic Nerve by Femoral Cerclage Wire: Illustrative Case and Management Strategy.
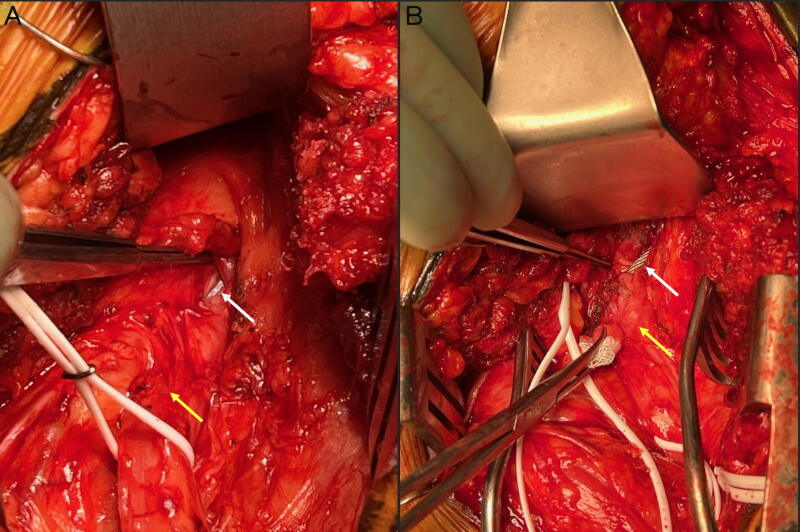
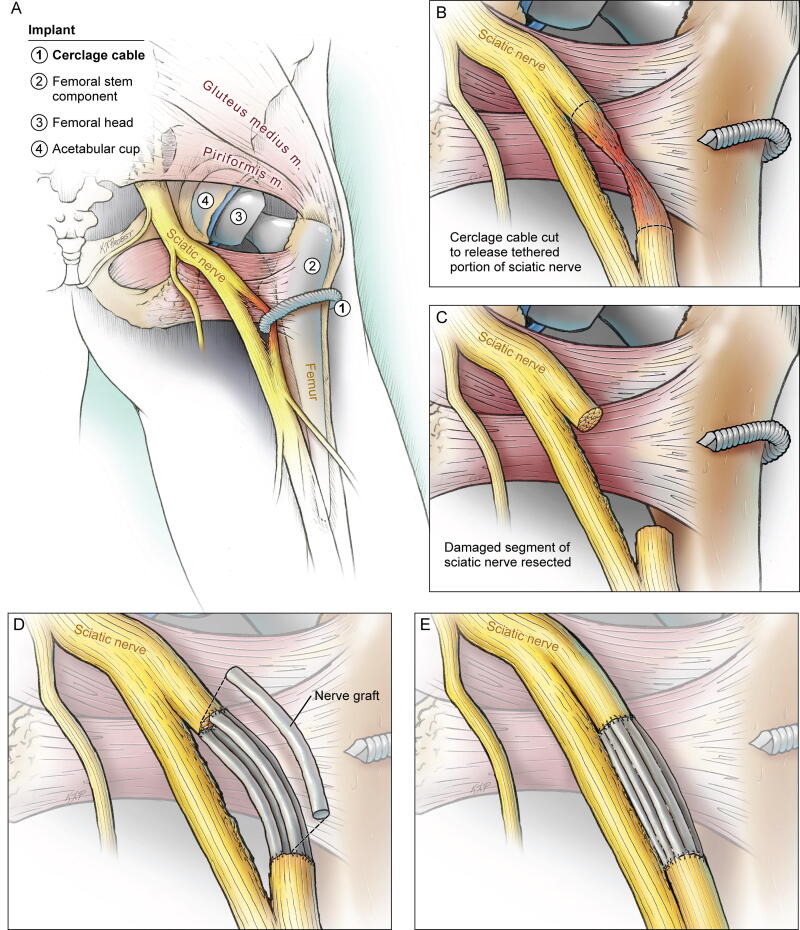
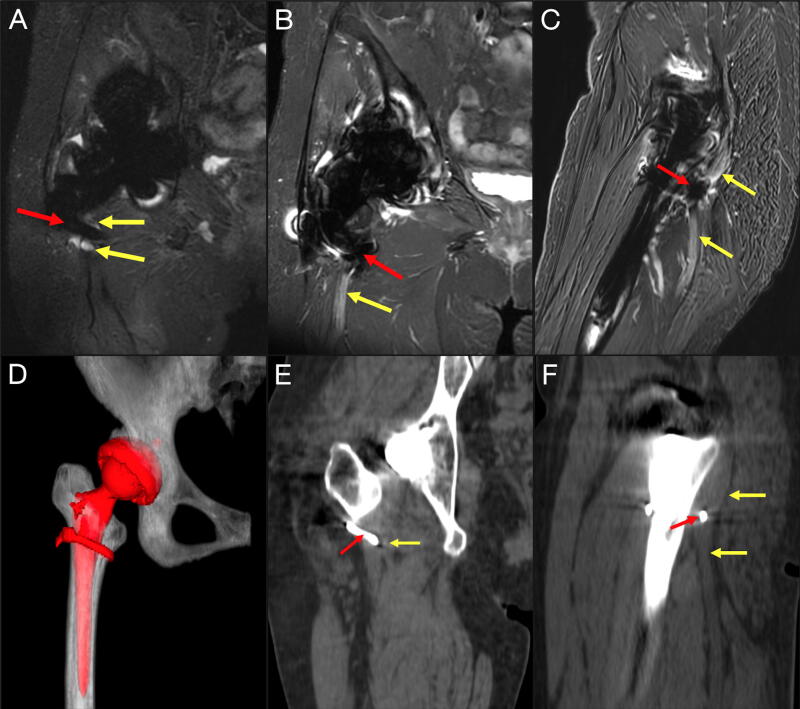
Sciatic nerve injury associated with total hip arthroplasty (THA) confers chronic and progressive disability. Mechanisms of injury are heterogeneous and management nuances are often case-specific. We discuss a Sunderland Type 4 sciatic nerve transection by femoral cerclage wire from prior THA to highlight optimal clinical strategies when approaching complex cases. A 65-year-old woman presented to the neurosurgery clinic with worsening, medically refractory right sciatic sensorimotor neuropathy that began 1 year after ipsilateral hip arthroplasty. Neurological examination detected weakness in ankle dorsiflexion/plantarflexion and foot inversion/eversion (motor scale 2-3/5), toe extension/flexion (1/5), foot numbness, and hyperesthesia. Electromyogram confirmed sciatic neuropathy. Magnetic resonance neurogram (MRN) showed a thickened right sciatic nerve abutting a femoral cerclage wire, which appeared contiguous on reconstructed computed tomography imaging. Intraoperatively, the wire was discovered to have clearly transected and remained lodged within the sciatic nerve, requiring orthopedic surgery consultation and wire cutdown at the transection site. The surrounding neuroma was excised and the defect was reconstructed using nerve allograft interposition. Intraoperative neurophysiology monitoring (IONM) signals remained stable. Radiographs confirmed uncomplicated wire disconnection. The patient was discharged home the next day and reported significant symptomatic relief at 1-month follow-up. Delayed presentation of sciatic nerve transection by femoral cerclage wire with ongoing neural compression is rare. The anatomy of injury can be high risk, impelling thoughtful operative planning in THA as well as neuroplasty cases. Strategies include preoperative MRN to evaluate the pathoanatomy of nerve injury, neurosurgery and orthopedic surgery comanagement, and multimodal IONM to reduce risks of intraoperative neural injury and optimize outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


