Olivier Massé, Noémie Maurice, Yu Hong, Claudia Mercurio, Catherine Tremblay, Lysane Senécal, Amélie Bernier-Jean, Nicolas Dugré, Gabriel Dallaire
{"title":"房颤维持性血液透析患者卒中预防策略的共享决策辅助(simplified - hd):一项混合方法研究","authors":"Olivier Massé, Noémie Maurice, Yu Hong, Claudia Mercurio, Catherine Tremblay, Lysane Senécal, Amélie Bernier-Jean, Nicolas Dugré, Gabriel Dallaire","doi":"10.1177/20543581241311077","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Recent atrial fibrillation guidelines recommend shared decision-making between clinicians and patients when choosing stroke-prevention therapies. Although decision aids improve patients' knowledge and decisional conflicts, there is no decision aid for stroke-prevention strategies in people with atrial fibrillation receiving hemodialysis.</p><p><strong>Objective: </strong>The objective was to develop and field test the first decision aid for Atrial Fibrillation in HemoDialysis (AFHD-DA) for stroke prevention in atrial fibrillation and hemodialysis.</p><p><strong>Design: </strong>This is a sequential 3-phase mixed-methods study following the International Patient Decision Aid Standards and the Ottawa Decision Support Framework.</p><p><strong>Setting: </strong>This study was conducted in 2 ambulatory hemodialysis centers in Montreal and Laval (Canada).</p><p><strong>Participants: </strong>Adults with atrial fibrillation receiving hemodialysis and clinicians (physicians, pharmacists, or nurse practitioners) involved in their care.</p><p><strong>Methods: </strong>In phase 1, we conducted systematic and 2 rapid reviews and formed the steering committee to pilot the first version of AFHD-DA. In phase 2, we refined the AFHD-DA through 4 rounds of focus groups and interviews, using a qualitative analysis of transcripts and a descriptive analysis of acceptability and usability scores. In phase 3, we field-tested the decision aid during 16 simulated clinical consultations. We assessed decisional conflict and patient knowledge using before-and-after paired <i>t</i>-tests and compared the proportion of patients with high decisional conflict using McNemar's test. We used the Ottawa Hospital preparation for decision-making scale and participants' feedback to evaluate how AFHD-DA facilitated shared decision-making.</p><p><strong>Results: </strong>We enrolled 8 patients and 10 clinicians in phase 2. The predefined usability and acceptability thresholds (68 and 66, respectively) were reached. Theme saturation was achieved in the fourth round of focus groups and interviews. Four major themes emerged: acceptability, usability, decision-making process, and scientific value of the decision aid. Sixteen patients and 10 clinicians field-tested the decision aid in phase 3. In clinical settings, AFHD-DA significantly decreased the mean decisional conflict score from 41.0 to 13.6 (<i>P</i> < .001) and the proportion of patients with decisional conflicts from 81.3 to 18.8% (<i>P</i> = .002). It improved the patients' mean knowledge score from 62.7 to 76.6 (<i>P</i> = .001), and 81% of patients and 90% of clinicians felt highly prepared for decision-making. Clinical consultations lasted, on average, 21 minutes (standard deviation = 8).</p><p><strong>Limitations: </strong>The main limitations were the low quality of existing literature, the small number of participants, and the absence of a control group.</p><p><strong>Conclusions: </strong>The decision aid facilitated time-efficient shared decision-making between clinicians and patients, improved patients' knowledge, and reduced decisional conflict around selecting a stroke-prevention strategy for patients with atrial fibrillation receiving hemodialysis.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581241311077"},"PeriodicalIF":1.5000,"publicationDate":"2025-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11843691/pdf/","citationCount":"0","resultStr":"{\"title\":\"Shared Decision-Making Aid for Stroke-Prevention Strategies in Patients With Atrial Fibrillation Receiving Maintenance Hemodialysis (SIMPLIFY-HD): A Mixed-Methods Study.\",\"authors\":\"Olivier Massé, Noémie Maurice, Yu Hong, Claudia Mercurio, Catherine Tremblay, Lysane Senécal, Amélie Bernier-Jean, Nicolas Dugré, Gabriel Dallaire\",\"doi\":\"10.1177/20543581241311077\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Recent atrial fibrillation guidelines recommend shared decision-making between clinicians and patients when choosing stroke-prevention therapies. Although decision aids improve patients' knowledge and decisional conflicts, there is no decision aid for stroke-prevention strategies in people with atrial fibrillation receiving hemodialysis.</p><p><strong>Objective: </strong>The objective was to develop and field test the first decision aid for Atrial Fibrillation in HemoDialysis (AFHD-DA) for stroke prevention in atrial fibrillation and hemodialysis.</p><p><strong>Design: </strong>This is a sequential 3-phase mixed-methods study following the International Patient Decision Aid Standards and the Ottawa Decision Support Framework.</p><p><strong>Setting: </strong>This study was conducted in 2 ambulatory hemodialysis centers in Montreal and Laval (Canada).</p><p><strong>Participants: </strong>Adults with atrial fibrillation receiving hemodialysis and clinicians (physicians, pharmacists, or nurse practitioners) involved in their care.</p><p><strong>Methods: </strong>In phase 1, we conducted systematic and 2 rapid reviews and formed the steering committee to pilot the first version of AFHD-DA. In phase 2, we refined the AFHD-DA through 4 rounds of focus groups and interviews, using a qualitative analysis of transcripts and a descriptive analysis of acceptability and usability scores. In phase 3, we field-tested the decision aid during 16 simulated clinical consultations. We assessed decisional conflict and patient knowledge using before-and-after paired <i>t</i>-tests and compared the proportion of patients with high decisional conflict using McNemar's test. We used the Ottawa Hospital preparation for decision-making scale and participants' feedback to evaluate how AFHD-DA facilitated shared decision-making.</p><p><strong>Results: </strong>We enrolled 8 patients and 10 clinicians in phase 2. The predefined usability and acceptability thresholds (68 and 66, respectively) were reached. Theme saturation was achieved in the fourth round of focus groups and interviews. Four major themes emerged: acceptability, usability, decision-making process, and scientific value of the decision aid. Sixteen patients and 10 clinicians field-tested the decision aid in phase 3. In clinical settings, AFHD-DA significantly decreased the mean decisional conflict score from 41.0 to 13.6 (<i>P</i> < .001) and the proportion of patients with decisional conflicts from 81.3 to 18.8% (<i>P</i> = .002). It improved the patients' mean knowledge score from 62.7 to 76.6 (<i>P</i> = .001), and 81% of patients and 90% of clinicians felt highly prepared for decision-making. Clinical consultations lasted, on average, 21 minutes (standard deviation = 8).</p><p><strong>Limitations: </strong>The main limitations were the low quality of existing literature, the small number of participants, and the absence of a control group.</p><p><strong>Conclusions: </strong>The decision aid facilitated time-efficient shared decision-making between clinicians and patients, improved patients' knowledge, and reduced decisional conflict around selecting a stroke-prevention strategy for patients with atrial fibrillation receiving hemodialysis.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"12 \",\"pages\":\"20543581241311077\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-02-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11843691/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581241311077\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241311077","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Shared Decision-Making Aid for Stroke-Prevention Strategies in Patients With Atrial Fibrillation Receiving Maintenance Hemodialysis (SIMPLIFY-HD): A Mixed-Methods Study.
Background: Recent atrial fibrillation guidelines recommend shared decision-making between clinicians and patients when choosing stroke-prevention therapies. Although decision aids improve patients' knowledge and decisional conflicts, there is no decision aid for stroke-prevention strategies in people with atrial fibrillation receiving hemodialysis.
Objective: The objective was to develop and field test the first decision aid for Atrial Fibrillation in HemoDialysis (AFHD-DA) for stroke prevention in atrial fibrillation and hemodialysis.
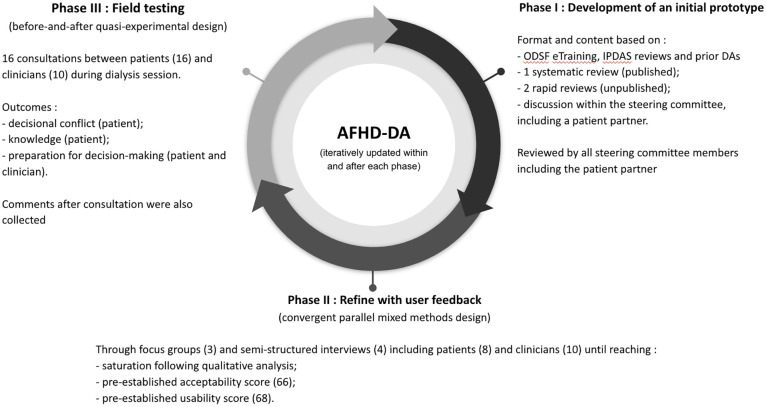
Design: This is a sequential 3-phase mixed-methods study following the International Patient Decision Aid Standards and the Ottawa Decision Support Framework.
Setting: This study was conducted in 2 ambulatory hemodialysis centers in Montreal and Laval (Canada).
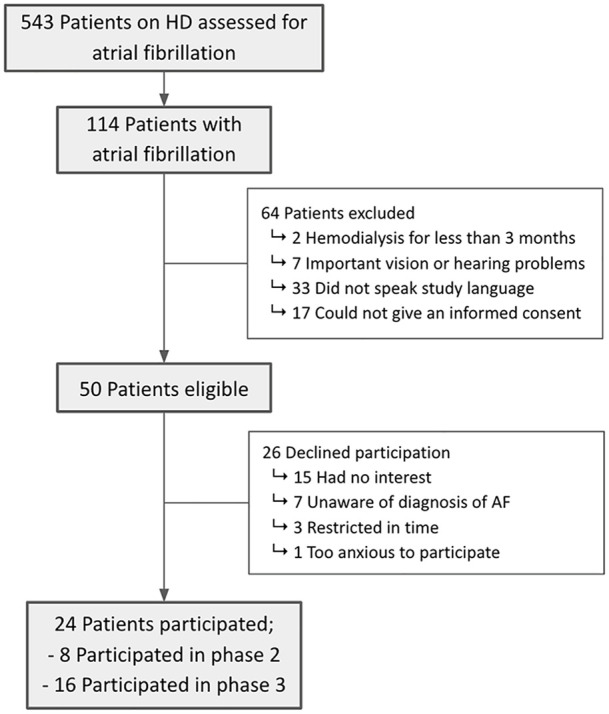
Participants: Adults with atrial fibrillation receiving hemodialysis and clinicians (physicians, pharmacists, or nurse practitioners) involved in their care.
Methods: In phase 1, we conducted systematic and 2 rapid reviews and formed the steering committee to pilot the first version of AFHD-DA. In phase 2, we refined the AFHD-DA through 4 rounds of focus groups and interviews, using a qualitative analysis of transcripts and a descriptive analysis of acceptability and usability scores. In phase 3, we field-tested the decision aid during 16 simulated clinical consultations. We assessed decisional conflict and patient knowledge using before-and-after paired t-tests and compared the proportion of patients with high decisional conflict using McNemar's test. We used the Ottawa Hospital preparation for decision-making scale and participants' feedback to evaluate how AFHD-DA facilitated shared decision-making.
Results: We enrolled 8 patients and 10 clinicians in phase 2. The predefined usability and acceptability thresholds (68 and 66, respectively) were reached. Theme saturation was achieved in the fourth round of focus groups and interviews. Four major themes emerged: acceptability, usability, decision-making process, and scientific value of the decision aid. Sixteen patients and 10 clinicians field-tested the decision aid in phase 3. In clinical settings, AFHD-DA significantly decreased the mean decisional conflict score from 41.0 to 13.6 (P < .001) and the proportion of patients with decisional conflicts from 81.3 to 18.8% (P = .002). It improved the patients' mean knowledge score from 62.7 to 76.6 (P = .001), and 81% of patients and 90% of clinicians felt highly prepared for decision-making. Clinical consultations lasted, on average, 21 minutes (standard deviation = 8).
Limitations: The main limitations were the low quality of existing literature, the small number of participants, and the absence of a control group.
Conclusions: The decision aid facilitated time-efficient shared decision-making between clinicians and patients, improved patients' knowledge, and reduced decisional conflict around selecting a stroke-prevention strategy for patients with atrial fibrillation receiving hemodialysis.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


