{"title":"儿童重症监护病房收治的自身免疫性炎症性风湿病儿童和青少年的死亡率","authors":"Tinnapat Buranapattama, Suwannee Phumeetham, Nuntawan Piyaphanee, Maynart Sukharomana, Sirirat Charuvanij","doi":"10.1186/s12969-025-01068-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aimed to describe the characteristics and outcomes of children and adolescents with autoimmune inflammatory rheumatic diseases (AIIRD) who were admitted to the pediatric intensive care unit (PICU). The accuracy of the Pediatric Risk of Mortality (PRISM) III and Pediatric Index of Mortality (PIM) 3 scores to predict the mortality were investigated.</p><p><strong>Methods: </strong>This was a retrospective cohort study. Children and adolescents with AIIRD aged ≤ 18 years who were admitted to the PICU at the largest university-based referral center in Thailand during July 2011 to June 2021 were included.</p><p><strong>Results: </strong>There were 122 PICU admissions from 74 patients; mean age of 12.0 ± 4.3 years, 74.3% female. Majority of AIIRD were systemic lupus erythematosus (SLE) (83.8%), followed by systemic juvenile idiopathic arthritis (5.4%), juvenile dermatomyositis (JDM) (2.7%) and microscopic polyangiitis (2.7%). The main cause of admission was combined infection and disease flare (29.5%). Pneumonia was the main site of infection. Acinetobacter baumanii was the most common causative agent. Macrophage activation syndrome occurred in 8 (6.5%) admissions. The mortality rate of PICU admissions was 14.8% from 18 deaths; 17 with SLE and 1 with JDM. Mechanical ventilation (aOR 24.07, 95%CI:1.33-434.91, P= 0.031), pneumothorax (aOR 24.08, 95%CI:1.76-328.86, P = 0.017 and thrombocytopenia (aOR 8.34, 95%CI:1.31-53.73, P = 0.025) were associated with mortality. The risk of mortality rate as predicted by the PRISM III score increased with a score ≥ 9. For the PIM 3 score, the risk of mortality increased if the score ≥ 3. The area under the ROC curve for the PRISM III and PIM 3 scores was 0.741 (95%CI: 0.633-0.849), P = 0.001 and 0.804 (95%CI: 0.685-0.924), P < 0.001, respectively. The model calibration using the Hosmer-Lemeshow goodness of fit test demonstrated a chi-square of 4.335, P = 0.826 for PRISM III and 7.987, P = 0.435 for PIM 3.</p><p><strong>Conclusion: </strong>SLE was the main AIIRD that required admission to the PICU. Mechanical ventilation, pneumothorax and thrombocytopenia were associated with mortality in pediatric patients with AIIRD. The PRISM III and PIM 3 scores demonstrated good calibration, while the PIM 3 score provided better discrimination ability in the prediction of mortality for pediatric AIIRD.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"23 1","pages":"20"},"PeriodicalIF":2.3000,"publicationDate":"2025-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11843957/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mortality in children and adolescents with autoimmune inflammatory rheumatic diseases admitted to the pediatric intensive care unit.\",\"authors\":\"Tinnapat Buranapattama, Suwannee Phumeetham, Nuntawan Piyaphanee, Maynart Sukharomana, Sirirat Charuvanij\",\"doi\":\"10.1186/s12969-025-01068-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study aimed to describe the characteristics and outcomes of children and adolescents with autoimmune inflammatory rheumatic diseases (AIIRD) who were admitted to the pediatric intensive care unit (PICU). The accuracy of the Pediatric Risk of Mortality (PRISM) III and Pediatric Index of Mortality (PIM) 3 scores to predict the mortality were investigated.</p><p><strong>Methods: </strong>This was a retrospective cohort study. Children and adolescents with AIIRD aged ≤ 18 years who were admitted to the PICU at the largest university-based referral center in Thailand during July 2011 to June 2021 were included.</p><p><strong>Results: </strong>There were 122 PICU admissions from 74 patients; mean age of 12.0 ± 4.3 years, 74.3% female. Majority of AIIRD were systemic lupus erythematosus (SLE) (83.8%), followed by systemic juvenile idiopathic arthritis (5.4%), juvenile dermatomyositis (JDM) (2.7%) and microscopic polyangiitis (2.7%). The main cause of admission was combined infection and disease flare (29.5%). Pneumonia was the main site of infection. Acinetobacter baumanii was the most common causative agent. Macrophage activation syndrome occurred in 8 (6.5%) admissions. The mortality rate of PICU admissions was 14.8% from 18 deaths; 17 with SLE and 1 with JDM. Mechanical ventilation (aOR 24.07, 95%CI:1.33-434.91, P= 0.031), pneumothorax (aOR 24.08, 95%CI:1.76-328.86, P = 0.017 and thrombocytopenia (aOR 8.34, 95%CI:1.31-53.73, P = 0.025) were associated with mortality. The risk of mortality rate as predicted by the PRISM III score increased with a score ≥ 9. For the PIM 3 score, the risk of mortality increased if the score ≥ 3. The area under the ROC curve for the PRISM III and PIM 3 scores was 0.741 (95%CI: 0.633-0.849), P = 0.001 and 0.804 (95%CI: 0.685-0.924), P < 0.001, respectively. The model calibration using the Hosmer-Lemeshow goodness of fit test demonstrated a chi-square of 4.335, P = 0.826 for PRISM III and 7.987, P = 0.435 for PIM 3.</p><p><strong>Conclusion: </strong>SLE was the main AIIRD that required admission to the PICU. Mechanical ventilation, pneumothorax and thrombocytopenia were associated with mortality in pediatric patients with AIIRD. The PRISM III and PIM 3 scores demonstrated good calibration, while the PIM 3 score provided better discrimination ability in the prediction of mortality for pediatric AIIRD.</p>\",\"PeriodicalId\":54630,\"journal\":{\"name\":\"Pediatric Rheumatology\",\"volume\":\"23 1\",\"pages\":\"20\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-02-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11843957/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Rheumatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12969-025-01068-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-025-01068-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
Mortality in children and adolescents with autoimmune inflammatory rheumatic diseases admitted to the pediatric intensive care unit.
Background: This study aimed to describe the characteristics and outcomes of children and adolescents with autoimmune inflammatory rheumatic diseases (AIIRD) who were admitted to the pediatric intensive care unit (PICU). The accuracy of the Pediatric Risk of Mortality (PRISM) III and Pediatric Index of Mortality (PIM) 3 scores to predict the mortality were investigated.
Methods: This was a retrospective cohort study. Children and adolescents with AIIRD aged ≤ 18 years who were admitted to the PICU at the largest university-based referral center in Thailand during July 2011 to June 2021 were included.
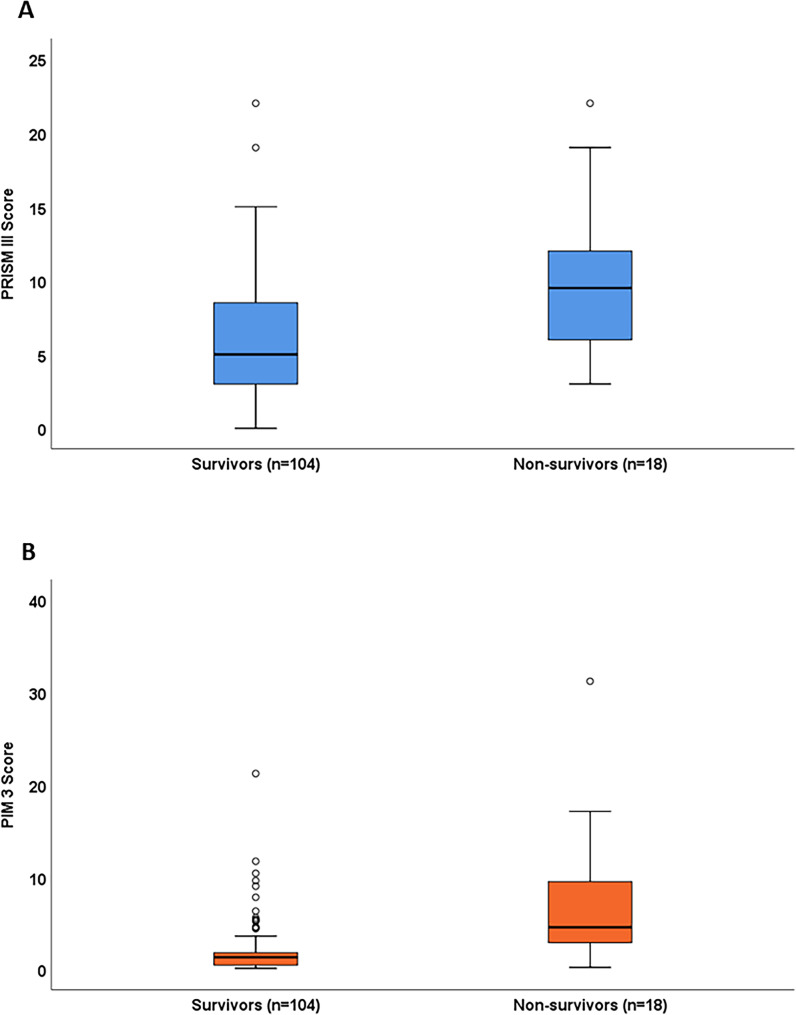
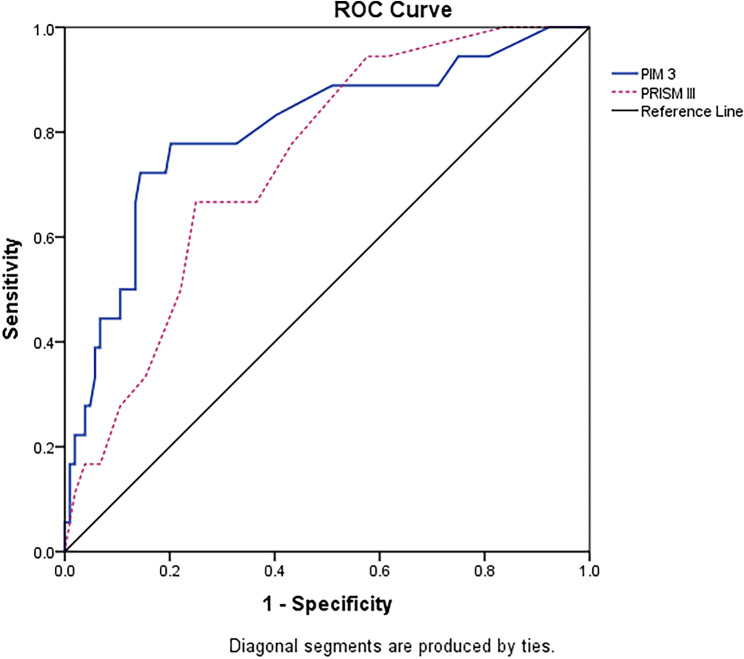
Results: There were 122 PICU admissions from 74 patients; mean age of 12.0 ± 4.3 years, 74.3% female. Majority of AIIRD were systemic lupus erythematosus (SLE) (83.8%), followed by systemic juvenile idiopathic arthritis (5.4%), juvenile dermatomyositis (JDM) (2.7%) and microscopic polyangiitis (2.7%). The main cause of admission was combined infection and disease flare (29.5%). Pneumonia was the main site of infection. Acinetobacter baumanii was the most common causative agent. Macrophage activation syndrome occurred in 8 (6.5%) admissions. The mortality rate of PICU admissions was 14.8% from 18 deaths; 17 with SLE and 1 with JDM. Mechanical ventilation (aOR 24.07, 95%CI:1.33-434.91, P= 0.031), pneumothorax (aOR 24.08, 95%CI:1.76-328.86, P = 0.017 and thrombocytopenia (aOR 8.34, 95%CI:1.31-53.73, P = 0.025) were associated with mortality. The risk of mortality rate as predicted by the PRISM III score increased with a score ≥ 9. For the PIM 3 score, the risk of mortality increased if the score ≥ 3. The area under the ROC curve for the PRISM III and PIM 3 scores was 0.741 (95%CI: 0.633-0.849), P = 0.001 and 0.804 (95%CI: 0.685-0.924), P < 0.001, respectively. The model calibration using the Hosmer-Lemeshow goodness of fit test demonstrated a chi-square of 4.335, P = 0.826 for PRISM III and 7.987, P = 0.435 for PIM 3.
Conclusion: SLE was the main AIIRD that required admission to the PICU. Mechanical ventilation, pneumothorax and thrombocytopenia were associated with mortality in pediatric patients with AIIRD. The PRISM III and PIM 3 scores demonstrated good calibration, while the PIM 3 score provided better discrimination ability in the prediction of mortality for pediatric AIIRD.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


