Alison E Simmons, Gebremedhin B Gebretekle, Robert Pless, Aleksandra Wierzbowski, Matthew Tunis, Ashleigh R Tuite
{"title":"加拿大儿童接种 13 价、15 价和 20 价肺炎球菌结合疫苗的比较:成本效用分析。","authors":"Alison E Simmons, Gebremedhin B Gebretekle, Robert Pless, Aleksandra Wierzbowski, Matthew Tunis, Ashleigh R Tuite","doi":"10.14745/ccdr.v51i23a02","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Two pneumococcal conjugate vaccines, covering 15 and 20 <i>Streptococcus pneumoniae</i> serotypes (Pneu-C-15 and Pneu-C-20, respectively), were recently approved for use in the Canadian paediatric population.</p><p><strong>Objective: </strong>To assess the cost-effectiveness of Pneu-C-15 and Pneu-C-20 in unvaccinated infants initiating routine pneumococcal vaccination, compared to the currently used 13-valent conjugate vaccine (Pneu-C-13).</p><p><strong>Methods: </strong>A static cohort model was used to estimate sequential incremental cost-effectiveness ratios (ICERs in 2022 Canadian dollars per quality-adjusted life year [QALY]) of Pneu-C-13, Pneu-C-15 and Pneu-C-20 in the paediatric population starting their primary series. Costs and outcomes were calculated over a 10-year time horizon at the program level and a lifetime time horizon at the individual level and discounted at a rate of 1.5% per year. We explored the impact of uncertainties in model parameters and assumptions in scenario and sensitivity analyses.</p><p><strong>Results: </strong>Routine use of Pneu-C-20 and, to a lesser extent, Pneu-C-15 is projected to reduce pneumococcal disease burden, compared to Pneu-C-13. Based on product cost assumptions, sequential ICERs for Pneu-C-15 and Pneu-C-20 were $58,800 and $135,200 per QALY gained from the health system perspective and $18,272 and $93,416 per QALY gained from the societal perspective, excluding indirect effects. A reduction in serotype-attributable disease due to indirect vaccine effects of 5% or greater resulted in ICERs below $30,000 per QALY gained for Pneu-C-15 and Pneu-C-20, with the optimal strategy determined by the magnitude and time to reach a reduction in pneumococcal disease.</p><p><strong>Conclusion: </strong>Both Pneu-C-15 and Pneu-C-20 are expected to increase QALYs in Canadian children compared to Pneu-C-13 and may be cost-effective interventions.</p>","PeriodicalId":94304,"journal":{"name":"Canada communicable disease report = Releve des maladies transmissibles au Canada","volume":"51 2-3","pages":"68-83"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842121/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of 13-, 15- and 20-valent pneumococcal conjugate vaccines in the paediatric Canadian population: A cost-utility analysis.\",\"authors\":\"Alison E Simmons, Gebremedhin B Gebretekle, Robert Pless, Aleksandra Wierzbowski, Matthew Tunis, Ashleigh R Tuite\",\"doi\":\"10.14745/ccdr.v51i23a02\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Two pneumococcal conjugate vaccines, covering 15 and 20 <i>Streptococcus pneumoniae</i> serotypes (Pneu-C-15 and Pneu-C-20, respectively), were recently approved for use in the Canadian paediatric population.</p><p><strong>Objective: </strong>To assess the cost-effectiveness of Pneu-C-15 and Pneu-C-20 in unvaccinated infants initiating routine pneumococcal vaccination, compared to the currently used 13-valent conjugate vaccine (Pneu-C-13).</p><p><strong>Methods: </strong>A static cohort model was used to estimate sequential incremental cost-effectiveness ratios (ICERs in 2022 Canadian dollars per quality-adjusted life year [QALY]) of Pneu-C-13, Pneu-C-15 and Pneu-C-20 in the paediatric population starting their primary series. Costs and outcomes were calculated over a 10-year time horizon at the program level and a lifetime time horizon at the individual level and discounted at a rate of 1.5% per year. We explored the impact of uncertainties in model parameters and assumptions in scenario and sensitivity analyses.</p><p><strong>Results: </strong>Routine use of Pneu-C-20 and, to a lesser extent, Pneu-C-15 is projected to reduce pneumococcal disease burden, compared to Pneu-C-13. Based on product cost assumptions, sequential ICERs for Pneu-C-15 and Pneu-C-20 were $58,800 and $135,200 per QALY gained from the health system perspective and $18,272 and $93,416 per QALY gained from the societal perspective, excluding indirect effects. A reduction in serotype-attributable disease due to indirect vaccine effects of 5% or greater resulted in ICERs below $30,000 per QALY gained for Pneu-C-15 and Pneu-C-20, with the optimal strategy determined by the magnitude and time to reach a reduction in pneumococcal disease.</p><p><strong>Conclusion: </strong>Both Pneu-C-15 and Pneu-C-20 are expected to increase QALYs in Canadian children compared to Pneu-C-13 and may be cost-effective interventions.</p>\",\"PeriodicalId\":94304,\"journal\":{\"name\":\"Canada communicable disease report = Releve des maladies transmissibles au Canada\",\"volume\":\"51 2-3\",\"pages\":\"68-83\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-02-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842121/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canada communicable disease report = Releve des maladies transmissibles au Canada\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14745/ccdr.v51i23a02\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canada communicable disease report = Releve des maladies transmissibles au Canada","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14745/ccdr.v51i23a02","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:两种肺炎球菌结合疫苗,分别覆盖15和20种肺炎链球菌血清型(分别为肺炎- c -15和肺炎- c -20),最近被批准用于加拿大儿科人群。目的:与目前使用的13价结合疫苗(肺炎- c -13)相比,评估未接种疫苗的婴儿开始常规肺炎球菌疫苗接种的肺炎- c -15和肺炎- c -20的成本效益。方法:采用静态队列模型估计在开始初级系列的儿科人群中,肺炎- c -13、肺炎- c -15和肺炎- c -20的顺序增量成本-效果比(ICERs,以2022加元/质量调整生命年[QALY]计算)。在项目层面上,成本和结果是在10年的时间范围内计算的,在个人层面上,成本和结果是在一生的时间范围内计算的,并以每年1.5%的比率贴现。我们在情景分析和敏感性分析中探讨了模型参数和假设中的不确定性的影响。结果:与肺炎- c -13相比,常规使用肺炎- c -20和在较小程度上使用肺炎- c -15预计可减少肺炎球菌疾病负担。基于产品成本假设,从卫生系统角度来看,肺部- c -15和肺部- c -20的连续ICERs分别为每个QALY获得58,800美元和135,200美元,从社会角度来看,每个QALY获得18,272美元和93,416美元,不包括间接影响。由于间接疫苗效应导致血清型可归因于疾病减少5%或更多,导致肺炎- c -15和肺炎- c -20的ICERs低于每QALY获得的30,000美元,最佳策略取决于减少肺炎球菌疾病的程度和时间。结论:与pneuc -13相比,pneuc -15和pneuc -20有望提高加拿大儿童的QALYs,并且可能是具有成本效益的干预措施。
Comparison of 13-, 15- and 20-valent pneumococcal conjugate vaccines in the paediatric Canadian population: A cost-utility analysis.
Background: Two pneumococcal conjugate vaccines, covering 15 and 20 Streptococcus pneumoniae serotypes (Pneu-C-15 and Pneu-C-20, respectively), were recently approved for use in the Canadian paediatric population.
Objective: To assess the cost-effectiveness of Pneu-C-15 and Pneu-C-20 in unvaccinated infants initiating routine pneumococcal vaccination, compared to the currently used 13-valent conjugate vaccine (Pneu-C-13).
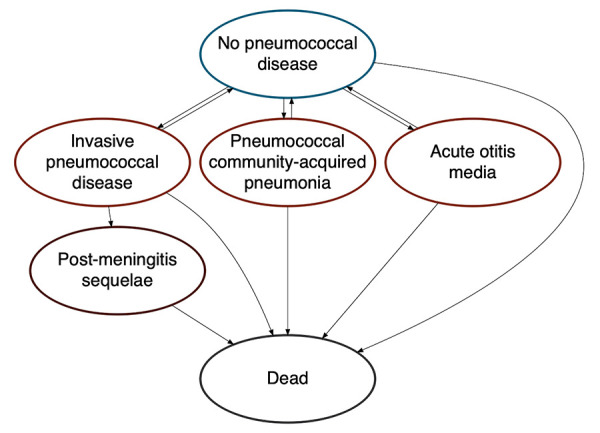
Methods: A static cohort model was used to estimate sequential incremental cost-effectiveness ratios (ICERs in 2022 Canadian dollars per quality-adjusted life year [QALY]) of Pneu-C-13, Pneu-C-15 and Pneu-C-20 in the paediatric population starting their primary series. Costs and outcomes were calculated over a 10-year time horizon at the program level and a lifetime time horizon at the individual level and discounted at a rate of 1.5% per year. We explored the impact of uncertainties in model parameters and assumptions in scenario and sensitivity analyses.
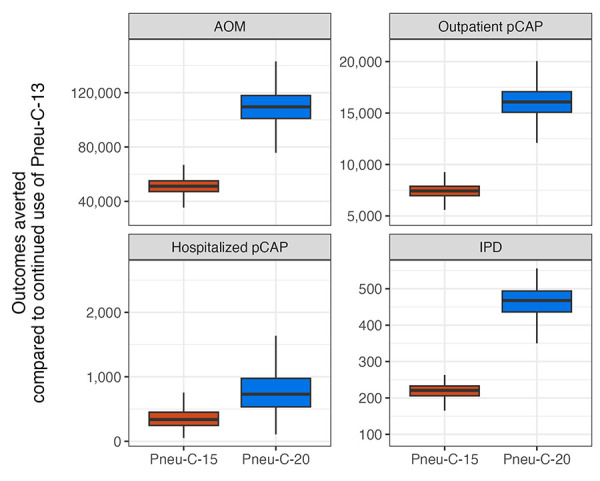
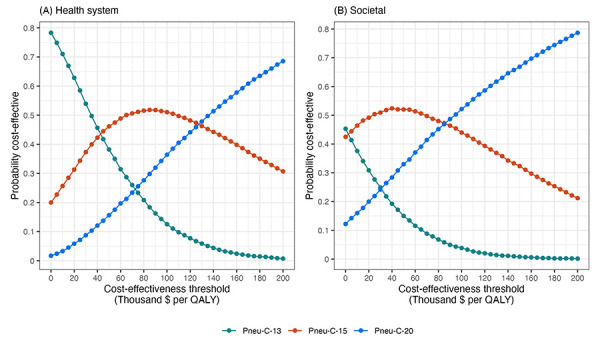
Results: Routine use of Pneu-C-20 and, to a lesser extent, Pneu-C-15 is projected to reduce pneumococcal disease burden, compared to Pneu-C-13. Based on product cost assumptions, sequential ICERs for Pneu-C-15 and Pneu-C-20 were $58,800 and $135,200 per QALY gained from the health system perspective and $18,272 and $93,416 per QALY gained from the societal perspective, excluding indirect effects. A reduction in serotype-attributable disease due to indirect vaccine effects of 5% or greater resulted in ICERs below $30,000 per QALY gained for Pneu-C-15 and Pneu-C-20, with the optimal strategy determined by the magnitude and time to reach a reduction in pneumococcal disease.
Conclusion: Both Pneu-C-15 and Pneu-C-20 are expected to increase QALYs in Canadian children compared to Pneu-C-13 and may be cost-effective interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


